Introduction
A bronchioloalveolar carcinoma (BAC) pattern is defined as growth of neoplastic cells along preexisting alveolar structures (lepidic growth) [1]. Although this pattern is a distinctive feature of BAC that is noninvasive adenocarcinoma, invasive adenocarcinomas often contain areas of BAC morphology at the tumor periphery. Numerous data over the past decade have demonstrated the heterogeneity of pulmonary adenocarcinomas in terms of clinical, radiologic, pathologic, and, in particular, molecular aspects [2,3]. This brought about the rationale for a change in the World Health Organization (WHO) classification of lung adenocarcinoma, culminating in a revision by the International Association for the Study of Lung Cancer, American Thoracic Society, and European Respiratory Society (IASLC/ATS/ERS) [3]. In this new classification, the term BAC has been abandoned, and new terms of adenocarcinoma in situ (AIS), minimally invasive adenocarcinoma (MIA), and lepidic predominant adenocarcinoma (LPA) are introduced. The most important issue is invasion. Although molecular and biological events responsible for this acquisition of invasiveness have been discussed in many reports [4-6], they remain to be elucidated.
Transforming growth factor β (TGFβ), a pleiotropic cytokine comprised of three isoforms in mammalian cells, is involved in a variety of biological processes, including cell proliferation and differentiation, wound healing, embryogenesis, and apoptosis. Function of TGFβs as tumor suppressors during early tumorigenesis, but also as mediators of tumor promoting effects in the later stages of cancer, has been demonstrated in clinical and mouse models [7,8]. Although several signaling pathways have been implicated in the mechanism of TGFβ action, precise timing and context by which TGFβ signaling functions alternatively in suppression of tumor growth or in promotion of tumor cell invasion remain unclear. Findings of a recent investigation in human lung adenocarcinoma cell lines indicated that TGFβ1 may promote invasion and metastasis via epithelial-to-mesenchymal transition (EMT). E-Cadherin, a cell-surface glycoprotein, is responsible for maintenance of intercellular connection. Loss of E-cadherin expression with subsequent reduction in cell-to-cell adhesion is a hallmark of EMT. Previous studies have reported involvement of TGFβ1 in regulation of E-cadherin [9,10]. However, the relationships between their expression profiles and morphology have not been reported in tumor progression of lung adenocarcinoma.
In the current study, we recategorized lung adenocarcinomas with and without lepidic growth according to the new classification system [3], and analyzed the expression of TGFβ1 and E-cadherin proteins in each subgroup in order to address the role of TGFβ1 and E-cadherin in tumor progression of pulmonary adenocarcinoma and to evaluate their differential expression in association with morphologic characteristics.
Materials and Methods
1. Patient characteristics
A total of 65 patients who underwent surgical resection for lung adenocarcinoma at the Catholic University St. Vincent's Hospital from January 1, 2005 to December 31, 2009 were included in this study. All tumors were staged according to the International Union against Cancer (UICC) guidelines of the 6th edition of the TNM classification of malignant tumors. Tumors with lepidic growth were histologically reclassified according to the amount of invasive component, as described recently by the new IASLC/ATS/ERS classification system [3]: 1) AIS (≤3 cm formerly BAC as defined by WHO [1] if there was no evidence of invasion; 2) MIA (formerly BAC with focal invasion) if there was a predominant lepidic pattern with an area of invasion comprising ≤5 mm within a tumor mass ≤3 cm; 3) LPA (formerly nonmucinous BAC pattern with >5 mm invasion). We categorized 65 adenocarcinomas into four groups: group 1, 2a, 2b, and 3. A summary of definitions for each group is shown in Table 1. This study protocol was approved by the Institutional Review Board (IRB) of St. Vincent's Hospital at The Catholic University of Korea (IRB no. VC12TIS10190). Informed consent was waived by the IRB. Clinical information was obtained through a computerized database of the tumor registry.
2. Immunohistochemical analysis
Whole tissue sections were obtained from 65 formalin-fixed, paraffin-embedded tumor specimens, and were analyzed for TGFβ1 and E-cadherin using immunohistochemical studies. Briefly, histology sections measuring 4 µm in thickness were deparaffinized in xylene, and rehydrated through a series of alcohols and water. Endogenous peroxidase activity was blocked by soaking the slides in 3% H2O2 at 45℃ for 10 minutes. For antigen retrieval, the sections were autoclaved in a citrate buffer (2.1 g/L, pH 6.0) for 15 minutes. The sections were then treated with a protein blocking reagent before incubation overnight at 4℃ with primary antibodies at a 1:100 dilution: anti-TGFβ1 (Santa Cruz Biotech, Santa Cruz, CA) and anti-E-cadherin (Cell Marque, Rocklin, CA). After extensive washing with Tris buffer, immunohistochemical staining was performed using the UltraVision LP detection system (Thermo Fisher Scientific, Fremont, CA). Diaminobenzidine was used as a chromogen and Meyer's hematoxylin was used as a nuclear counterstain.
Positive and negative controls were run in all series. Positive controls were breast carcinoma tissue for TGFβ1 and pituitary gland for E-cadherin. For negative controls, the primary antibody was omitted during processing. Immunohistochemical and pathological assessments were performed in a blind fashion by an experienced pathologist (J.Yoo). Expression for TGFβ1 was evaluated according to the percentage of tumor cells with immunoreactivity in their cytoplasm: +, if ≥ 10% of tumor cells were stained; -, if no detectable expression or <10% of tumor cells were stained [11]. The membrane showed strong E-cadherin staining and the cytoplasm showed weak staining. E-Cadherin expression was considered positive when >90% of tumor cells showed membranous staining [12].
3. Statistical analysis
Statistical analyses were performed using the SPSS ver. 19.0 (SPSS Inc., Chicago, IL). Correlations between histologic subtypes and immunohistochemical expressions were estimated using the chi-square and Fisher's exact tests. A p-value of <0.05 was considered statistically significant.
Results
Clinical and pathologic data are shown in Table 2. Of the patients, 28 were men and 37 were women. The median age at diagnosis was 66 years (range, 33 to 82 years). Twenty-one patients were former or current smokers, and 44 were never-smokers. Forty-one patients had stage I disease, six had stage II disease, 16 had stage III disease, and two had stage IV disease. Upon pathology review, 20 tumors were classified into group 1, nine into group 2a, 17 into group 2b, and 19 into group 3. Of a total of 65 lesions, noninvasive elements were observed in 46 specimens, and invasive elements were observed in 45 (Table 3).
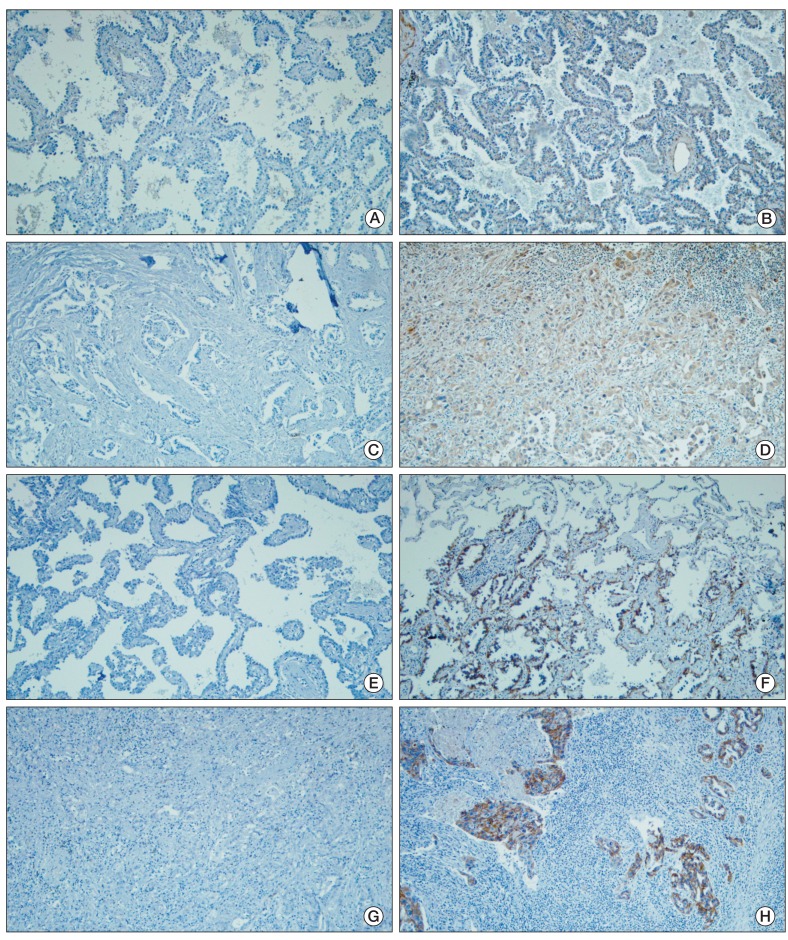
Negative and positive controls showed the expected results. More frequent expression of TGFβ1 was observed in invasive foci than in BAC component (87% vs. 46%), and the difference was statistically significant (p=0.001) (Table 3, Fig. 1A-D). In contrast, the prevalence of E-cadherin expression was significantly high in areas with noninvasive component when compared with that in invasive foci (65% vs. 38%, p=0.009) (Fig. 1E-H). Expression of TGFβ1 and E-cadherin showed significant correlation in noninvasive components (p=0.022), but not in invasive foci (p=0.385) (Table 4). In order to further characterize different subgroups of lung adenocarcinoma with and without lepidic growth, we examined the expression of TGFβ1 and E-cadherin proteins in the noninvasive component and invasive component for each group, respectively. More frequent expression of TGFβ1 was observed in the noninvasive component of group 2b (14/17, 82%) than in that of either group 1 (5/20, 25%) or group 2a (2/9, 22%) (Table 5). The differences were statistically significant: group 1 vs. group 2a+group 2b (p=0.014), and group 1+group 2a vs. group 2b (p=0.008). TGFβ1 expression in invasive foci was demonstrated in 100% of group 2a (9/9), 88% of group 2b (15/17), and 79% of group 3 (15/19); no significant correlations were observed between the following groups: group 2a vs. group 2b+group 3 (p=0.323), and group 2a+group 2b vs. group 3 (p=0.377). However, in group 2a, expression of TGFβ1 was observed in all invasive elements, but in two of nine noninvasive elements (p=0.002). Immunoreactivity with anti-E-cadherin in noninvasive elements was exhibited in 70% (14/20) of group 1, 67% (6/9) of group 2a, and 59% (10/17) of group 2b. The frequency was lower in group 2b than in group 1+group 2a, however, it did not reach statistical significance (p=0.489). No association was found between group 1 and group 2a+group 2b (p=0.550). E-cadherin expression in invasive foci was observed in 78% (7/9) of group 2a, 35% (6/17) of group 2b, and 21% (4/19) of group 3. Significantly higher frequency was observed in group 2a than in group 2b+group 3 (p=0.017). The difference in E-cadherin expression between group 2a+group 2b and group 3 approached statistical significance (p=0.065).
Discussion
To date, little is known about the sequence of molecular events and morphologic changes in development of invasive lung adenocarcinoma. In particular, it has not yet been determined which of the two precedes the other in stepwise progression. We compared the expression status of TGFβ1 and E-cadherin proteins between the noninvasiveand invasive components of pulmonary adenocarcinomas with varying degrees of invasion. The major findings of our study are as follows: 1) the frequency of TGFβ1 overexpression was significantly increased in invasive foci, whereas E-cadherin expression was more common in noninvasive elements; 2) TGFβ1 expression showed inverse correlation with E-cadherin expression in noninvasive components; 3) up-regulation of TGFβ1 occurs not only before loss of E-cadherin but also before the structural destruction of the alveolar wall by invasive tumor cells.
Overexpression of TGFβ1 has been reported in lung cancer, particularly in association with tumor progression. Hasegawa et al. [13] reported a negative correlation of TGFβ1 with patient survival in non-small cell lung carcinoma (NSCLC). In their study, TGFβ1 protein levels were measured in surgically resected NSCLC tissues using enzyme-linked immunosorbent assay, and showed correlation with tumor angiogenesis. Other researchers have demonstrated by immunohistochemistry the significance of TGFβ1 overexpression in metastasis and prognosis of pulmonary adenocarcinoma, however, they did not divide the tumors into subgroups or mention whether BACs were included in the samples [14,15].
Molecular studies in different subtypes of lung adenocarcinoma are rather limited. In a study of small early lung adenocarcinoma reported by Aoyagi et al. [6], a significant increase in the incidence of loss of heterozygosity (LOH) was observed with a more invasive morphology: 16.7% of Noguchi type A tumors (localized bronchioloalvelar carcinoma [LBAC]) vs. 39.3% of Noguchi type B tumors (LBAC with alveolar collapse) vs. 96.2% of Noguchi type C tumors (LBAC with active fibroblastic proliferation). In addition, in type C tumors, LOH was observed more frequently in central fibrotic areas than in peripheral BAC areas. This finding suggests that tumor cells in fibrotic regions are molecularly different from those in peripheral BAC regions, and are more genetically altered and malignant. Using DNA microarray analysis, Borczuk et al. [16], who examined gene expression signatures associated with invasiveness in three subgroups of pulmonary adenocarcinoma (BAC, mixed adenocarcinoma with BAC, and invasive carcinoma), reported that the gene expression signature of purely invasive tumors was distinct from those of other adenocarcinomas, and the repression of type II TGFβ receptor may act as a significant determinant of lung adenocarcinoma invasiveness. In the current study, we examined lung adenocarcinomas encompassing a spectrum of invasion using immunohistochemistry to demonstrate TGFβ1 status in vivo. In agreement with previous reports [13-16], our data showed a high frequency of TGFβ1 expression in invasive foci compared with noninvasive foci, which supports the involvement of TGFβ1 up-regulation in tumor invasion. However, of LPAs, TGFβ1 expression showed a significant increase at similar frequencies in both noninvasive and invasive elements (82% vs. 88%). In addition, in the noninvasive components of each subgroup, a significant difference was observed between LPA and AIS or MIA; expression of TGFβ1 was much more frequent in LPA than in the other two subgroups. This finding suggests that tumor cells of noninvasive areas of LPA are morphologically similar to but molecularly different from those of AIS and MIA. This observation is important because TGFβ1 up-regulation appears to occur before morphologic destruction of the alveolar wall by invasion of tumor cells. Consistently high incidence of TGFβ1 expression in the invasive components of each subgroup further supports TGFβ1 up-regulation as an early event in the invasive process. Therefore, detection of TGFβ1 overexpression in small biopsy specimens showing adenocarcinoma with pure lepidic growth may have the potential for assumption of stromal invasion somewhere within the tumor and may be of great value in discriminating an AIS from a lepidic pattern of growth within an otherwise invasive adenocarcinoma. Western blotting of micro-dissected tumor samples from each component of each subgroup is currently in progress in our laboratory for validation.
Negative correlation between E-cadherin expression and invasiveness has been well documented in various cancers. In keeping with previous data [12,17], findings of our study demonstrated that loss of E-cadherin was increased as lung adenocarcinoma underwent histologic progression. E-Cadherin expression showed inverse correlation with TGFβ1 expression. In addition, no significant change in E-cadherin expression, but a marked increase in the rate of TGFβ1 expression, was detected in the noninvasive elements of LPA. These findings provide morphologic evidence that loss of E-cadherin occurs after TGFβ1 up-regulation, and that TGFβ1 down-regulates E-cadherin. Studies demonstrating involvement of TGFβ1 in down-regulation of E-cadherin, various signaling pathways of which have been implicated for possible mechanisms, have been reported [9,10,18]. Findings from a recent investigation in lung cancer cells demonstrated regulation of TGFβ-induced EMT by miR-23a through suppression of E-cadherin [9]. Further work on the biological control mechanism through EMT is needed in pulmonary adenocarcinoma subclasses in order to attain a better understanding of the sequential alterations of TGFβ1 and E-cadherin that may have morphological associations.
Conclusion
The current study demonstrated significant differences in TGFβ1 and E-cadherin expression between the noninvasive and invasive components of lung adenocarcinoma, indicating involvement of both TGFβ1 and E-cadherin proteins in tumor progression. Of noninvasive elements of each group, LPA exhibited TGFβ1 expression more frequently than AIS or MIA. In addition, despite being morphologically noninvasive, TGFβ1 expression was detected in noninvasive areas of LPA as compared to the incidence observed in invasive regions of each group. These findings suggest that TGFβ1 up-regulation is an early event in the invasive process, preceding structural destruction of the alveolar wall by invasion of tumor cells. Conduct of additional large-scale studies is warranted; the results of such investigation may be helpful in assessment of invasiveness in small biopsy specimens of pure lepidic growth.