Introduction
Despite of substantial advancements in the diagnosis and treatment technologies for cancer, cancer remains a prominent global burden, ranking among the most severe chronic illnesses worldwide. The global burden of disease study revealed that, in 2013, there were 14.9 million reported cancer incidence cases and 8.2 million cancer-related fatalities on a global scale [1]. In South Korea, in 2016, approximately 220,000 individuals were newly diagnosed with cancer, and around 78,000 died from cancer [2].
Several studies reported that there is socioeconomic inequity not only in the treatment of cancer but also in its incidence [3-10]. Several research conducted in Europe have indicated that individuals with low socioeconomic status tend to exhibit higher cancer incidence compared to individuals with high socioeconomic status [6-8].
South Korea is a nation with relatively low financial burdens regarding cancer diagnosis and treatment. The National Health Insurance (NHI) mandates that all citizens enroll in health insurance and provides financial assistance through the medical aid (MA) for those unable to afford medical insurance premiums, Consequently, South Korea achieved universal health coverage (UHC) [11]. Both the NHI and the MA in South Korea are encouraged to get regular cancer screening every 2 years. The out-of-pocket expenses for cancer screening are minimal, with the NHI covering up to 10% of the cost, and the MA offering screening at no cost to promote early cancer detection. Once a cancer diagnosis is confirmed, individuals with cancer are only required to bear 5% of their medical expenses.
The National Cancer Registry is very efficient and provides national cancer statistics. The National Cancer Registry provides highly accurate and detailed information on cancer incidence, mortality, and survival rates by cancer type, age group, sex, and region, including personal information such as patient’s social security number, address, and occupation, as well as various clinical information such as surveillance, epidemiology, and end results stage, metastasis, and differentiation, as well as date and cause of death and type of treatment.
However, this data does not include a variable to categorize the income level of patients, making it difficult to identify differences by economic level, which is one of the important factors in cancer incidence and mortality. The NHI claims data contains information on healthcare utilization related to the occurrence of cancer diseases and information on the type of health insurance coverage, which may indirectly reflect the income of cancer patients. Although more sophisticated results can be obtained by combining the National Cancer Registry data and the NHI claims data through additional work, we utilized the NHI claims data for efficient production of data and securing recent information. Because of the high correlation between the National Cancer Registry data and the NHI claims data on cancer incidence, the NHI claims data can be used to compare health disparities between the NHI beneficiaries and the MA recipients.
In previous studies utilizing the National Cancer Registry in South Korea, the nationwide cancer incidence is well-documented, but there is a lack of data regarding the socioeconomic status. Therefore, we aim to investigate the impact of socioeconomic status on cancer incidence using the NHI claims data. This study aims to investigate under the UHC whether: (1) there exists inequality in cancer incidence based on socioeconomic status, particularly insurance types and geographic regions; (2) whether such inequality is increasing; and (3) whether inequality exists in cancer treatment facilities based on socioeconomic status.
Materials and Methods
1. Data sources
To define patients with newly diagnosed cancer between 2011 and 2021, we used the NHI claims data of the National Health Insurance Service from 2005 through 2022, with a washout period of 5 years and a subsequent 1-year follow-up period to define episodes for patients in 2021. The NHI claims data contains information about patients (age, sex, type of insurance, diagnosis and treatment history, etc.) This is representative of data from almost all citizens, including the NHI and the MA patients [12,13].
Furthermore, we used the National Health Insurance Service’s annual health insurance and medical aid beneficiaries from 2011 to 2021. These statistics include the number of beneficiaries for the NHI and the MA by province, age, and sex at the end of each year [14].
2. Definitions
All inpatient and outpatient claim with a primary diagnosis of C00-C96 according to the Korean Standard Classification of Diseases and Causes of Death-8 (KCD-8) and a special benefit code for registered cancer patients (V193) were extracted and considered as medical utilization due to cancer. All cancers were categorized as the 10 most diagnosed cancers in Korea based on the National Cancer Registry Statistics 2019, and the rest were categorized as other cancers. The 10 cancers included thyroid cancer (C73), lung cancer (C33-C34), colorectal cancer (C18-C20), stomach cancer (C16), breast cancer (C50), prostate cancer (C61), liver cancer (C22), pancreatic cancer (C25), gallbladder and biliary tract cancer (C23-C24), and kidney cancer (C64) [15].
We constructed episodes of patients’ healthcare use with data classified by cancer type to define a newly diagnosed cancer case. The first episode by year established between 2011 and 2021 was defined as a newly diagnosed cancer case (new claim for major diagnosis of C code and V193; special certification for cancer) in the year if there was no healthcare use due to the same cancer in the previous 5 years.
The hospital type of the first diagnosis was defined as the type of hospital used by the patient in the first episode of healthcare use due to specific cancer. It was classified into tertiary hospitals, general hospitals, hospitals, and clinics.
Geographic regions were defined based on the residence of patients diagnosed with new cancer and categorized into 17 provinces according to the administrative divisions of the Korean Ministry of the Interior and Safety.
3. Statistical analysis
General characteristics and the hospital type of the first diagnosis are presented as mean and standard deviation or number and percentage. The age-sex standardized cancer incidence rates by cancer type and year according to the type of insurance and the age-sex standardized cancer incidence rate by cancer type and province in 2021 according to the type of insurance were presented as the number of diagnosed cancer cases per 100,000 population of beneficiaries. Age standardization was performed using 10-year age groups, except that age standardization by region was done for those under age 60 and over age 60 due to few occurrences per cell. To determine the trend in cancer incidence over time by a different type of insurance, a log-linear Poisson regression model was used to compare the annual percentage change (APC). The odds ratio (OR) with 95% confidence intervals was also calculated using the NHI group as a reference to compare the risk of new cancer incidence between two health insurance types. The statistical significance level was set to 0.05. All statistical analyses in this study were calculated using SAS software ver. 9.4 (SAS Institute Inc., Cary, NC).
Results
1. General characteristics of cancer patients in Korea
The trend of total cancer incidence increased from 255,971 cases in 2011 to 325,772 cases in 2021. The cancers that have increased the most are, in order, breast cancer, prostate cancer, lung cancer, colorectal cancer, pancreatic cancer, kidney cancer, and gallbladder cancer. Cancers whose incidence has plateaued or declined are thyroid cancer, stomach cancer, and liver cancer. Breast cancer cases were 18,362 and 32,541 in 2011 and 2021, lung cancer cases were 22,166 and 31,637 in 2011 and 2021, and colorectal cancer cases were 28,905 and 35,258 in 2011 and 2021. Among total cancer cases, thyroid cancer had the highest incidence and decreasing trend, with 41,700 cases in 2011 to 37,166 cases in 2021. Stomach cancer cases were 33,368 and 31,517 in 2011 and 2021, and liver cancer cases were 18,455 and 17,668 in 2011 and 2021.
By age group, the number and proportion of total cancer cases were prominent in 50-59 years, 60-69 years, and 70-79 years age group, while the proportion of total cancer cases was less than 2% in the ≤ 29 years age group. In addition, the proportion of sex was similar between male and female, about 95% of total cancer cases were covered by the NHI, and about 5% were the MA recipients. The general characteristics of the study subjects are shown in Tables 1, 2 and S1 Table.
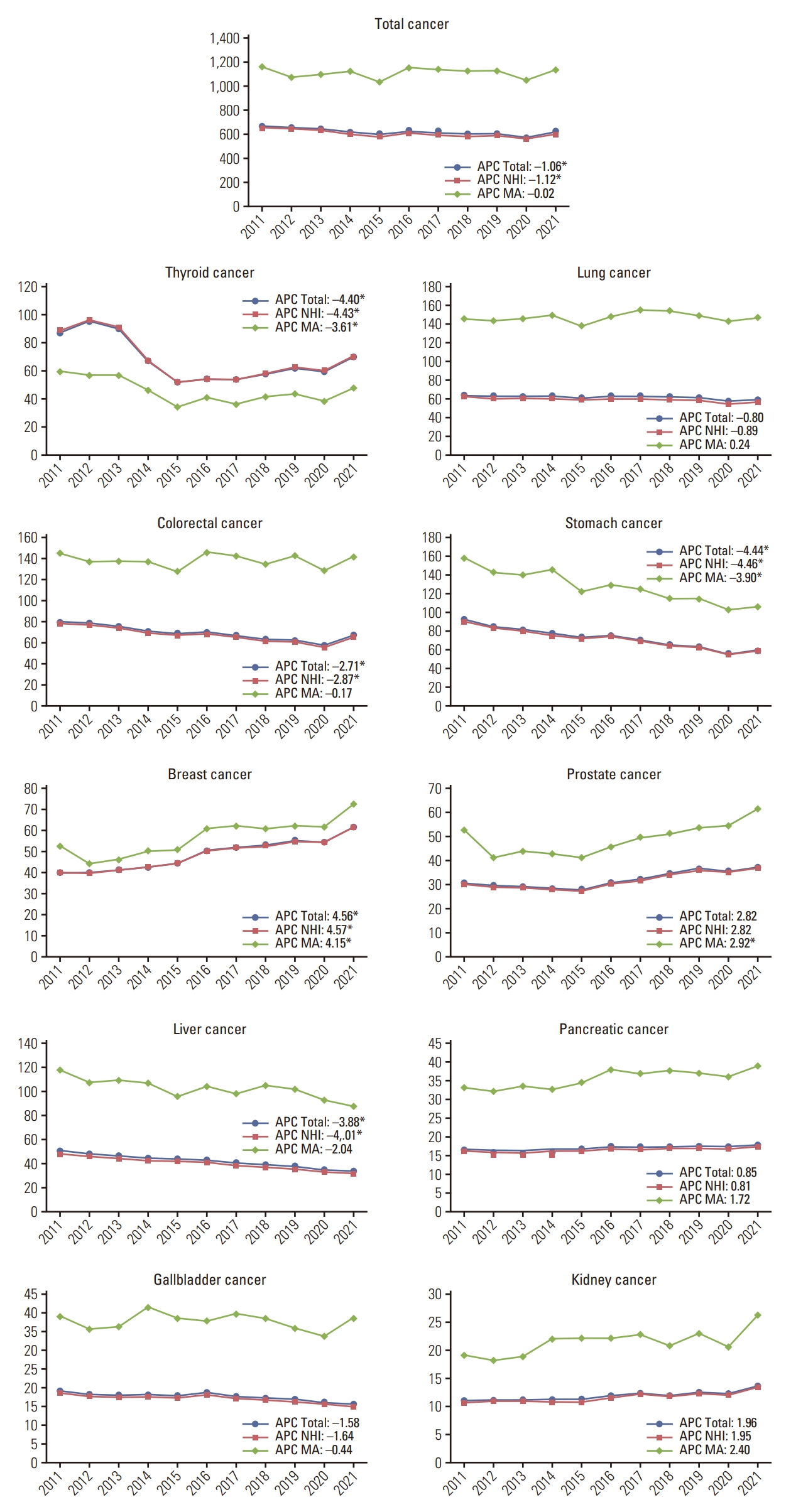
2. Age-sex standardized total cancer incidence by insurance type
As shown in Fig. 1 and S2 Table, The total cancer incidence rate showed an increasing trend, as did the NHI and the MA group. The gap between the NHI group and the MA group has widened from 2011 to 2021. The gap was lowest in 2012, with 434.1 cases per 100,000 population, and highest in 2016 at 550.1 cases per 100,000 population. By insurance type, the MA group had the higher cancer incidence rate than the NHI group. The total incidence rate of the NHI decreased from 652.0 cases per 100,000 population in 2011 to 600.4 cases per 100,000 population, whereas the total incidence rate of the MA decreased from 1,162.1 cases per 100,000 population in 2011 to 1,137.3 cases per 100,000 population. The absolute difference of total cancer incidence rate was 510.1 cases per 100,000 population in 2011 and 536.9 cases per 100,000 population in 2021. The APC in total cancer in total population was –1.06%-point, with –1.12%-point, and –0.02%-point in the NHI and the MA groups. The incidence of all types of cancer was higher in the MA group, except thyroid cancer. The incidence of liver cancer and stomach cancer was in a decreasing pattern in the NHI group, –3.88%-point and –4.44%-point, respectively.
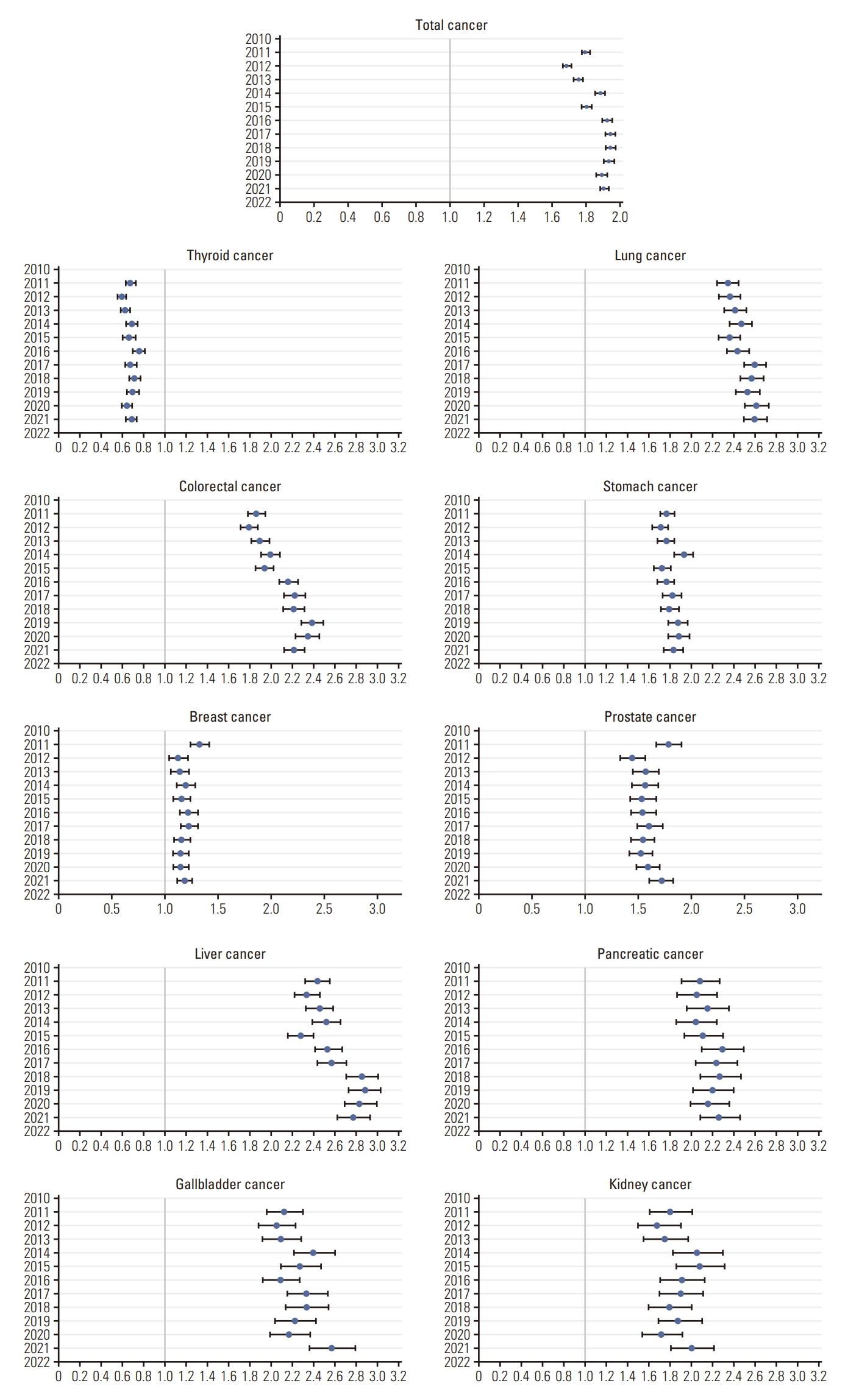
3. The OR of cancer incidence by insurance type
As Fig. 2 and S3 Table show the OR of cancer incidence by insurance type, the risk of total cancer incidence raised from 2011 to 2021. The OR of total cancer incidence showed an increasing pattern, with 1.79 (95% confidence interval [CI], 1.77 to 1.82), and 1.90 (95% CI, 1.88 to 1.93) in 2011 and 2021, respectively. The risk of all types of cancer incidence except thyroid cancer was significantly higher in the MA group than in the NHI group which is the reference. Cancers that have shown an increasing trend of the OR were lung cancer, colorectal cancer, stomach cancer, liver cancer, pancreatic cancer, gallbladder cancer, and kidney cancer. The OR of liver cancer was the highest among 10 types of cancer, 2.43 (95% CI, 2.31 to 2.54) in 2011 and 2.76 (95% CI, 2.61 to 2.92) in 2021. A decreasing trend of the OR was shown in breast cancer and prostate cancer. The OR of breast cancer was 1.32 (95% CI, 1.23 to 1.41), 1.18 (95% CI, 1.11 to 1.25) in 2011 and 2021. Only the OR of thyroid cancer incidence was less than 1. The OR was 0.67 (95% CI, 0.63 to 0.72) and 0.68 (95% CI, 0.63 to 0.73) in 2011 and 2021, respectively.
4. Disparities in hospital type of first diagnosis in cancer
In the MA group, the proportion of general hospitals was higher than the proportion of tertiary hospitals, with 61.4% of general hospitals and 28.5% of tertiary hospitals in 2011. However, the gap between general hospitals and tertiary hospitals has narrowed, with 38.7% of general hospitals and 54.0% of tertiary hospitals in 2021. Fig. 3 and S4-S6 Tables show the proportion of the type of hospital where patients were first diagnosed with cancer. The proportion was highest in tertiary hospitals, followed by general hospitals, hospitals, and local clinics in the NHI group. The sum of proportion of hospitals and local clinics was less than 10% in both groups. Since 2017, the proportion of tertiary hospitals for the first cancer diagnosis in the MA group has increased, however, it is still approximately 10% different from the NHI group.
5. Regional disparities in cancer incidence by insurance type
All regions showed differences in cancer incidence by insurance type. The cancer incidence rate was higher in the MA group than in the NHI group in every province. Fig. 4 and S7 Table show the regional disparities in cancer incidence by insurance type in 2021. Nationwide total cancer incidence rates were 605.4 cases per 100,000 population. Nationwide cancer incidence rates in the NHI and the MA groups were 589.9 cases per 100,000 population and 1,133.1 cases per 100,000 population. Disparities between insurance types also vary by region, with most provinces showing gap of approximately two-to-one between the NHI and the MA groups, while some provinces showed a smaller gap. Busan had the highest overall cancer rate at 646.1 cases per 100,000 population, while Jeju had the lowest overall cancer rate at 570.4 cases per 100,000 population.
Discussion
This study is the first paper to examine health inequities in relation to cancer incidence between the NHI beneficiaries and the MA recipients over the last decade in Korea. Cancer incidence has increased overall, and this trend was found in both the NHI group and the MA group. However, we found that cancer incidence was higher in the MA group than in the NHI group, and that the gap was widening. We also found that regional differences in cancer incidence still exist and are getting worse.
In addition, the risk of cancer incidence showed the same pattern as cancer incidence rates. The OR was higher in the MA group than in the NHI group. The OR of total cancer incidence was 1.79 (95% CI, 1.77 to 1.82) and 1.90 (95% CI, 1.88 to 1.93) in 2011 and 2021. Only the OR for thyroid cancer was conversely lower in the MA group, at 0.67 (95% CI, 0.63 to 0.72) and 0.68 (95% CI, 0.63 to 0.73) in 2011 and 2021, respectively. The reason why thyroid cancer tended to be different from other cancers is due to specific characteristic of thyroid cancer and thyroid cancer patients. Mortality of thyroid cancer is exceptionally low compared to other cancers, and thyroid cancer is known to be more affected by high socioeconomic factors such as income. People with high income tend to use more medical services than people with low income and are more at risk of overutilization [16-19]. High-income patients tend to be screened with more sensitive tests, and such tendency may lead to earlier diagnosis, increasing the possibility of overdiagnosis [19-21]. Such characteristics of thyroid cancer patients may have influenced the results that thyroid cancer has the highest number of patients of all cancers.
Assuming that even within the same region there are differences in the choice of higher level of care for socioeconomic reasons, we analyzed whether there were differences by type of initial diagnosis. The proportion of the type of hospital where patients were first diagnosed with cancer was different between the NHI and the MA groups. More than 60% of cancer incidence in the NHI beneficiaries was diagnosed at tertiary hospitals and around 30% at general hospitals. On the other hand, general hospitals were where ≥ 60% of cancer cases of the MA recipients were diagnosed between 2011 and 2016. This represents that the NHI beneficiaries could afford to pay more medical expenses while the MA recipients are financially vulnerable. However, in the MA group, the proportion of cancer diagnosis at tertiary hospitals increased from 28.5% in 2011 to 54.0% in 2021, while the proportion at general hospitals decreased from 61.4% in 2011 to 38.7% in 2021. These changes have been significant since 2017 for most cancers. We could possibly interpret this result as enhanced cancer coverage by the NHI. Under the health insurance coverage enhancement policy implemented since 2017, the upper limit of health insurance deductibles paid by the lowest 50% of income earners was reduced to 10% of their annual income. In addition to expanding rebates for low-income earners, the catastrophic medical expense support program, which covers therapeutic out-of-pocket medical expenses, was expanded from four serious diseases to all diseases, and the maximum amount of support was raised from KRW 20 million to KRW 30 million (USD 15,000 to USD 24,000).
In Korea, when a person is diagnosed with cancer of any type, the NHI covers 95% of medical expenses. Cancer patients pay only 5% of total cancer treatment expenses regardless of their health coverage. Cancer patients burden 5% of treatment expenses from out-of-pocket, therefore we may assume that cancer patients in the MA group feel less burdened by treatment costs, resulting in an increased proportion of tertiary hospitals in the first diagnosis of cancer. Despite an increase in the proportion of the MA patients diagnosed with cancer at tertiary hospitals, it was still about 10% lower than in the NHI group, and disparity still existed.
This study has some limitations. First, we used only cancer incidence as the outcome variable in this study. Health inequity would be ideal if it did not exist. However, unfortunately, inequity exists in the real world. Accurately measuring the magnitude of inequity is important. Therefore, choosing appropriate health inequity indicators is inevitable to measure health inequity. Four perspectives are considered when conducting research regarding cancer: treatment, mortality, screening, and stage. In this study, we could not afford to take cancer treatment, cancer mortality, and stage as outcome variables due to data structure. However, cancer incidence may be appropriate outcome variable in Korea. As stated above, with the low cost of treatment, there would be less reason for newly diagnosed cancer patients not to have medical treatment. Further research would be necessary to evaluate health disparities in cancer using other outcome variables such as treatment, mortality, stage, etc. Second, our results cannot provide information regarding the impact of coronavirus disease 2019 (COVID-19) on cancer patients in 2020 and 2021. As no conclusive evidence of carcinogenesis of COVID-19 has been established, we ruled out the risk of COVID-19. Third, while it is common to use cancer registry data to study cancer incidence or mortality, we were unable to use a variable for type of health insurance, which is the minimum variable to distinguish the economic level that is the main interest of this study. Instead, we used health insurance claims data, which can be used to manipulatively define new cancers through healthcare use by the total population. By using the primary diagnosis and a special benefit code for cancer, the accuracy of the data can be improved and considered reliable. Seo et al. [22] investigated that cancer incidence rates between the National Cancer Registry and the NHI claims data were very similar, with 363.1 cases per 100,000 population in the NHI claims data and 361.9 cases per 100,000 population in the National Cancer Registry data from 2005-2008.
In terms of future policy recommendations, it would be ideal if the National Cancer Registry data included an indicator of income. Currently, there are no income indicators in the National Cancer Registry data, so we are forced to use the NHI claims data. If it is not possible to add an income indicator to the National Cancer Registry data, it is essential to cooperate with relevant organizations to link the NHI claims data.
In conclusion, this study investigated that socioeconomic disparities in cancer incidence have worsened by health coverage, region, and over the study period. Nevertheless, increased health coverage may have influenced the proportion of tertiary hospitals in the MA group. Understanding these disparities is crucial for implementing of public health policies to reduce health inequality.