Introduction
Changes in hepatic contour that mimic cirrhosis radiographically, but lack the classic pathological attributes of cirrhosis, are referred to as pseudocirrhosis [1]. Features of portal hypertension, such as portosystemic venous collaterals and ascites, as well as hepatic surface nodularity can be seen on computed tomography (CT). Pseudocirrhosis has been described previously in patients with cancer with metastases to the liver, both in those who underwent prior systemic chemotherapy and those who did not. In particular, it has been reported almost exclusively in patients with breast cancer with liver metastases [2-4]. We report on a case of a patient with breast cancer with liver metastases who developed cirrhotic changes during disease progression. We report here on the histopathological findings and some issues to consider in pseudocirrhosis.
Case Report
A 47-year-old woman visited our hospital in January 2003 because of a painful right breast mass with skin dimpling. On initial evaluation, chest CT revealed the presence of a heterogeneous enhancing breast mass measuring 9 cm with skin invasion and multiple conglomerated lymph nodes in the right axillary area. In addition, multiple metastatic pleural masses with malignant pleural effusion and mediastinal lymph node enlargement were also observed. A bone scan showed increased uptake in the sternum and right sixth anterior rib. There was no evidence of liver metastases on the initial CT scan (Fig. 1A and B). Fine-needle aspiration cytology of the breast mass showed atypical malignant cells. Accordingly, she was diagnosed with stage IV right breast cancer with multiple pleural and bone metastases. She subsequently received palliative chemotherapy with docetaxel and epirubicin. Follow-up CT scan performed after four cycles of chemotherapy showed partial regression of the breast mass and multiple metastatic masses in the pleura and axillary area. She then underwent palliative total mastectomy of her right breast because of an ulcerated skin lesion. Pathological examination showed invasive ductal carcinoma with nuclear grade 2 and lymphatic and perineural invasion. Immunohistochemistry studies showed positive staining for the estrogen receptor (ER) protein, progesterone receptor protein, and human epidermal growth factor receptor 2 (HER2) (score 3). She received two additional cycles of chemotherapy with docetaxel and epirubicin. A follow-up CT scan showed stable disease and she then started taking tamoxifen (20 mg daily) in July 2003.
Two years later, in November 2005, a surveillance breast ultrasound showed an irregular circumscribed mass measuring 1 cm on theright mastectomy site. The patient underwent a wide local excision and pathology confirmed an invasive ductal carcinoma. Although previous metastatic lesions showed stable disease, a new chest wall lesion had developed; therefore, her treatment was switched from tamoxifen to the non-steroidal aromatase inhibitor anastrozole. At that time, she was postmenopausal, based on her serum follicle-stimulating hormone levels. In January 2007, a bone scan showed new increased uptake in the right second rib, the third anterior rib, and the right acetabulum. She had progressive disease of the bone; therefore, capecitabine (an oral prodrug of 5-fluorouracil; 2,500 mg/m2/day) was started (two weeks on, one week off). After nine cycles of chemotherapy, she had stable disease and was off chemotherapy for approximately four years with no evidence of progression.
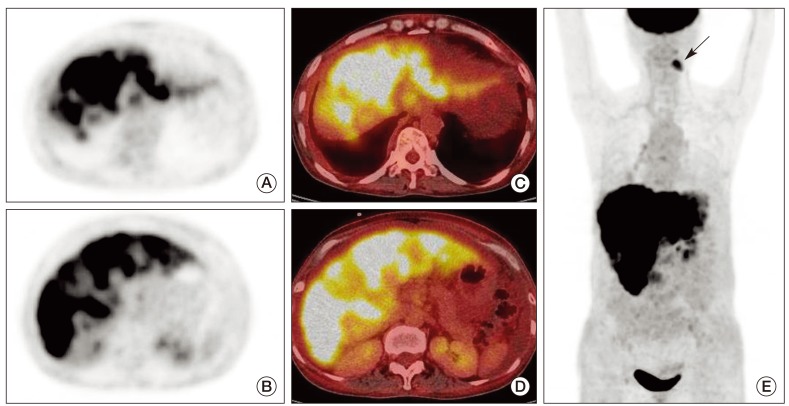
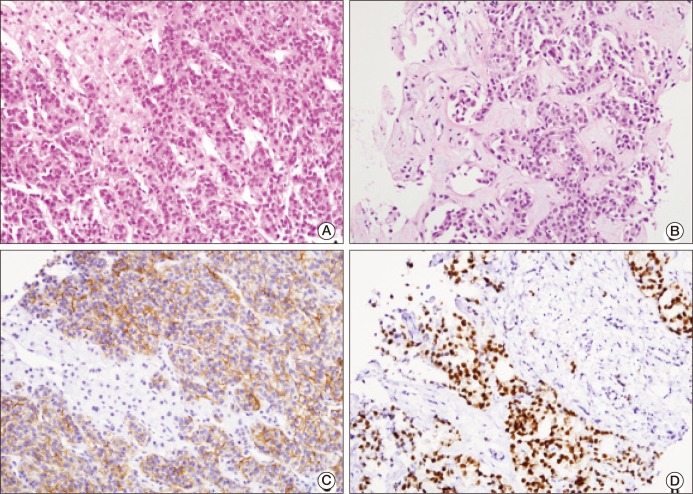
However, follow-up CT scan performed in June 2011 showed multiple newly developed peripheral enhancing nodules in the liver (Fig. 1C and D). She received six cycles of chemotherapy until November 2011, and CT scan showed that her metastatic hepatic lesions were stable. Since then, her chemotherapy has been discontinued because of grade 4 neutropenia and osteomyelitis of the mandible. Four months later, follow-up CT scan showed ill-defined heterogeneous enhancing lesions in the entire liver with surface nodularity. The liver had a nodular contour consistent with cirrhosis, as well as moderate ascites (Fig. 1E and F). F18 fluorodeoxyglucose (FDG) positron emission tomography/computed tomography (PET-CT) also showed disseminated and innumerable lesions throughout almost the entire liver with increased FDG uptake (maximum standardized uptake value [SUVmax], 7.3), suggesting diffuse liver metastasis (Fig. 2A-E). Palliative chemotherapy with docetaxel and epirubicin was started again. Endoscopy showed grade 3 large esophageal varices with a red color sign. She denied a history of liver disease, alcohol use, and risk factors for viral hepatitis. Serologies for viral or autoimmune etiologies of cirrhosis were negative and the serum level of alpha-fetoprotein was normal. An ultrasound-guided liver biopsy was performed in order to confirm the cause of the cirrhotic changes. Pathological examination showed that the hepatic parenchyma was diffusely infiltrated by poorly differentiated carcinoma cells. Hepatocytes were almost replaced by carcinoma cells and extensive fibrosis between clusters of cancer cells was observed (Fig. 3A and B). Immunohistochemical staining was positive for gross cystic disease fluid protein-15, MOC 31, ER, and HER2 (score 3), but negative for hepatocytes (Fig. 3C and D). Follow-up PET-CT showed progression of liver metastases with increased FDG uptake (SUVmax, 9.0) since the scan performed in June 2011. Therefore, we concluded that the hepatic metastases from breast cancer had progressed and led to cirrhotic changes in the liver.
Subsequently, her chemotherapy regimen was changed to trastuzumab and docetaxel. However, bleeding of esophageal varices occurred on the sixth day after initiation of chemotherapy, and hepatic failure progressed gradually. Therefore, the patient decided to discontinue chemotherapy.
Discussion
Cirrhosis is the end result of liver injury characterized by distortion of the hepatic architecture by extensive fibrosis and formation of regenerative nodules [5]. Cirrhosis is defined by its typical pathological features: 1) presence of regenerating nodules of hepatocytes and 2) presence of bridging fibrosis between these nodules [5]. CT findings of cirrhosis usually include diffuse hepatic surface nodularity and/or signs of portal hypertension such as splenomegaly, ascites, or portosystemic varices [6].
The term 'pseudocirrhosis' is used in the following cases: radiographic findings that resemble macronodular cirrhosis, but in which histopathological specimens fail to show the typical findings of cirrhosis [1]. The most frequently reported cause of pseudocirrhosis is breast cancer with liver metastases treated with chemotherapy; however, cirrhotic changes have also been reported in hepatic metastasis of a variety of cancers, including pancreatic cancer, esophageal cancer, small-cell lung cancer, and thyroid cancer [7-10]. The exact prevalence of pseudocirrhosis is not known. Qayyum et al. [1] reported follow-up CT results of 91 patients undergoing chemotherapy for breast cancer metastatic to the liver. They found that 16 (17%) patients showed diffuse nodularity of hepatic contour and eight (9%) patients showed signs of portal hypertension on serial CT [1]. Another study reported that various degrees of hepatic capsular retractions (ranging from 1 to 10 mm in depth) were observed in 29 (50%) of 58 patients with hepatic metastases from breast cancer [11].
The precise mechanism underlying development of pseudocirrhosis remains unclear. Based on previous studies, the causes of pseudocirrhosis in the setting of cancer have been classified according to two categories: 1) hepatic response to chemotherapeutic agents and 2) fibrosis combined with metastatic infiltrating tumors [4]. The first category is assumed to be a result of the hepatotoxic effect of systemic chemotherapy or a response to chemotherapy by tumor tissues [4]. This is independent from progression of hepatic metastases. Sonnenblick et al. [3] reported that five patients with breast carcinoma that was metastatic to the liver who had undergone chemotherapy and hormonal therapy developed pseudocirrhosis, despite a decrease in the size of their liver lesions. Hepatic histology in this setting is consistent with nodular regenerative hyperplasia with subsequent compression and atrophy of intervening parenchyma without fibrosis. Systemic chemotherapy can result in hepatic capsular retraction by tumor shrinkage and subsequent scar formation around the treated metastases, thus resembling macronodular cirrhosis [4,7]. Alternatively, nodular regenerative hyperplasia in response to chemotherapy-induced hepatic injury has been proposed as the mechanism of pseudocirrhosis [2]. Young et al. [2] reported on the pathological findings of 22 patients who had findings of pseudocirrhosis on CT. Fifteen patients had diffuse capsular retraction and seven patients had focal retraction. Six of the seven patients for whom tumor tissue could be obtained had nodular regenerative hyperplasia without fibrosis [2].
Another form of pseudocirrhosis occurs in cases in which hepatic histology shows evidence of extensive fibrosis representing a profound desmoplastic response to the infiltrating tumor [3,12]. Nascimento et al. [12] reported that two patients with pseudocirrhosis exhibited severe desmoplastic fibrosis and extensive tumor infiltration. In our case, we also confirmed diffuse infiltration of tumor cells and extensive fibrosis that developed during progression of liver metastases.
There are some issues related to pseudocirrhosis. First, cirrhotic changes may hamper interpretation of the evaluation of disease response during CT imaging. Both progression and regression of liver metastases can cause cirrhotic changes [1]. Currently, histological evaluation of liver biopsy specimens is critical for determining whether chemotherapeutic response or liver metastasis is the cause of pseudocirrhosis; however, this is an invasive procedure. In our case, a PET-CT scan showed progression of liver metastases with increased FDG uptake consistent with pathological findings. However, Sass et al. [4] reported different results regarding the role of PET-CT scan in the liver of a patient with autopsy evidence of diffuse infiltration by tumor cells. In their case of diffuse desmoplastic metastatic breast cancer simulating cirrhosis, PET-CT scans showed inhomogeneous uptake consistent with cirrhosis, but no focal areas of increased uptake suggestive of FDG-avid malignancy. Therefore, further studies of the role of PET-CT scan in evaluation of the response to chemotherapy in patients with pseudocirrhosis are needed. Second, there is a need for awareness of the risk of hepatic decompensation and the complication of portal hypertension. The clinical manifestations of portal hypertension, such as hepatic encephalopathy and variceal bleeding, which can bringon a life threatening condition, can be similar to those seen in classic cirrhosis. Therefore, these patients should be monitored carefully for progression of hepatic failure. In addition, early recognition and appropriate management of these complications are necessary. Careful selection of chemotherapeutic agents with consideration for hepatic dysfunction is also required. Third, some unresolved challenges remain, such as the relationship between any individual agent and development of pseudocirrhosis (which is more common in breast cancer than in other malignancies) and the relationship between the clinicopathological characteristics of breast cancer and pseudocirrhosis. Fennessy et al. [11] reported that hepatic capsular retraction in breast cancer with liver metastasis was associated with larger metastases and both an increase and a decrease in the size of subjacent lesions. However, it is unrelated to lesion number, histopathology, receptor status, or chemotherapeutic regimen. Therefore, further studies are required in order to address these problems and to determine the impact of changes in liver on patient survival and for development of appropriate strategies for treatment of patients with pseudocirrhosis. In conclusion, pseudocirrhosis can occur in breast cancer patients with liver metastasis treated by chemotherapy. In this setting, accurate assessment of treatment response in hepatic lesions can be difficult. Histopathological examination and PET-CT may be helpful in determining the direction of treatment. Appropriate management of portal hypertension, as well as treatment of the cancer, are also important.