Impact of T-Cell Engagers on COVID-19–Related Mortality in B-Cell Lymphoma Patients Receiving B-Cell Depleting Therapy
Article information

Abstract
Purpose
B-cell depleting therapies, including T-cell engager (TCE), are increasingly used for patients with hematologic malignancies, including during the coronavirus disease 2019 (COVID-19) pandemic. We aimed to evaluate the relationship between TCE therapy and COVID-19–related outcomes among patients with COVID-19 and B-cell lymphomas receiving B-cell depleting therapy.
Materials and Methods
This retrospective cohort study included patients with B-cell lymphoma, who were admitted to Seoul National University Hospital with COVID-19 between September 2021 and February 2023, and received B-cell depleting therapy before COVID-19 diagnosis. Multivariable logistic regression was used to identify factors associated with severe to critical COVID-19 and COVID-19–related mortality.
Results
Of 54 patients with B-cell lymphomas and COVID-19 who received B-cell depleting therapy, 14 were treated with TCE (TCE group) and 40 with rituximab (RTX group). COVID-19–related mortality was higher in the TCE group than in the RTX group (57.1% vs. 12.5%, p=0.002). In multivariable analyses, TCE therapy (adjusted odds ratio [aOR], 7.08; 95% confidence interval [CI], 1.29 to 38.76; p=0.024) and older age (aOR, 1.06; 95% CI, 1.00 to 1.13; p=0.035) were associated with severe to critical COVID-19. TCE therapy (aOR, 8.98; 95% CI, 1.48 to 54.40; p=0.017), older age (aOR, 1.13; 95% CI, 1.02 to 1.26; p=0.022), and prior bendamustine therapy (aOR, 7.78; 95% CI, 1.17 to 51.65; p=0.034) were independent risk factors for COVID-19–related mortality.
Conclusion
B-cell lymphoma patients treated with TCE had significantly worse outcomes from COVID-19 than those treated with RTX. TCE therapy should be used with caution in B-cell lymphoma patients during the COVID-19 epidemic.
Introduction
Increased risk from and poor outcomes of coronavirus disease 2019 (COVID-19) in patients with hematologic malignancies have been reported since the early days of the current pandemic [1,2]. Moreover, several studies have reported that patients with lymphoma treated using B-cell depleting therapy experience persistent COVID-19 pneumonia, for up to as long as 1 year [3,4]. Further, among patients with non-Hodgkin lymphoma, anti-CD20 therapy was associated with a higher risk of mortality due to COVID-19 [5].
Anti-CD20 therapies, such as rituximab (RTX), are widely used to treat B-cell malignancies, such as diffuse large B-cell lymphoma, follicular lymphoma, and mantle cell lymphoma [6]. Although anti-CD20 therapy has been reported to be associated with poor COVID-19 outcomes, most studies were conducted in the early COVID-19 pandemic before mass COVID-19 vaccination, emergence of the Omicron variant, and introduction of the use of T-cell engagers (TCEs) [5].
TCEs targeting CD3 on T-cells and B-cell markers were developed recently and are currently undergoing clinical trials as potential treatments for relapsed or refractory non-Hodgkin lymphoma [7,8]. These new TCE immunotherapies are theoretically expected to have more immunosuppressive effects than other B-cell depleting treatments; however, little is known about the effects of TCE treatment on COVID-19 outcomes.
In this retrospective cohort study, we examined the relationship between TCEs and COVID-19–related mortality among hospitalized patients with COVID-19 and B-cell lymphoma treated with B-cell depleting therapy.
Materials and Methods
1. Study design and population
This was a retrospective cohort study of patients with B-cell lymphoma aged ≥ 18 years, who were admitted to Seoul National University Hospital with COVID-19 between September 2021 and February 2023, and had been treated with B-cell depleting therapy before being diagnosed with COVID-19. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infections were confirmed by real-time reverse transcription polymerase chain reaction.
Patients were divided into two groups according to the use of TCEs: those treated with TCE (the TCE group) or those treated with other B-cell depleting therapy (all were treated with RTX; the RTX group). The following TCEs were used: CD20×CD3 bispecific antibodies (epcoritamab, mosunetuzumab, glofitamab, and odronextamab) and a CD22×CD3 bispecific antibody (JNJ-75348780). The following chemotherapy regimens, including RTX plus cyclophosphamide, doxorubicin, vincristine, and prednisone; RTX plus methotrexate, vincristine, and procarbazine; and RTX plus bendamustine, were mainly used for patients in the RTX group.
2. Data collection and definitions
Data were collected from patient medical records, including demographic information, underlying comorbidities, Eastern Cooperative Oncology Group performance status, and lymphoma-related data, including type, stage, status, history of B-cell depleting therapy, and prior anti-lymphoma therapy. COVID-19–related data, including the date of COVID-19 diagnosis, clinical course of COVID-19, vaccination status, duration of isolation, and treatment for COVID-19, were also obtained. COVID-19 severity was classified according to the National Institutes of Health guidelines [9]; mild and moderate COVID-19 cases were defined as non-severe. COVID-19–related mortality was defined as death due to active COVID-19 during isolation and hospitalization. In-hospital mortality included death that occurred during hospitalization after recovery from COVID-19 if the patients remained hospitalized for reasons other than COVID-19. Survival time was censored as of March 21, 2023.
Being fully vaccinated was defined as more than 2 weeks after completion of recommended doses of COVID-19 vaccines. Lymphoma was diagnosed based on the 2016 World Health Organization (WHO) classification of lymphoid neoplasms [10], and Ann Arbor staging at diagnosis and response assessment were collected using the Lugano classification system [11]. Other than Ann Arbor staging, lymphoma-related variables, including status, history of B-cell depleting therapy, and prior anti-lymphoma therapy, were collected when patients had COVID-19. For variables related to B-cell depleting therapy, in the TCE group, the total duration, cycles, and interval from last B-cell depleting therapy to COVID-19 diagnosis were collected based on TCE, even if patients in the TCE group had been previously treated with RTX. In the Republic of Korea, the dominant variant of SARS-CoV-2 from September 2021 to December 2021 was considered the Delta variant, while the Omicron variant has been considered dominant since January 2022.
3. Statistical analysis
Continuous variables are presented as median with interquartile range (IQR) and categorical variables are presented as numbers and percentages. A Student’s t-test or Mann-Whitney U test was used to compare continuous variables, and a chi-squared test or Fisher’s exact test was used to compare categorical variables, as appropriate. Risk factors for severe to critical COVID-19 and COVID-19–related mortality were evaluated using multivariable logistic regression analysis. Variables with p < 0.10 in univariate analysis were included in the multivariable analysis using backward stepwise logistic regression.
Surviving patients were censored at the time of last clinic visit or 1 year after COVID-19 diagnosis in survival curves. COVID-19–related and overall survival were estimated using Kaplan-Meier curves and comparisons between two groups conducted by stratified log-rank test. For all statistical analyses, two-sided p < 0.05 was considered statistically significant. Statistical analyses were performed using SPSS Statistics ver. 26.0 (IBM Corp., Armonk, NY).
Results
1. Patient characteristics
A total of 54 patients with COVID-19 and B-cell lymphoma who received B-cell depleting therapy were included in the analysis. Of the 54 patients, 14 (25.9%) were classified into the TCE group and 40 (74.1%) into the RTX group. Of the 14 patients in the TCE group, seven were treated with epcoritamab, four with mosunetuzumab, one with glofitamab, one with odronextamab, and one with JNJ-75348780. Median (IQR) age of patients in the TCE group was older than that in the RTX group (75 [69–79] vs. 64 [58–74] years, p=0.013) (Table 1). Vaccination status and underlying comorbidities did not differ significantly between the two groups, and there were no significant differences in lymphoma subtype or Ann Arbor staging.

Clinical characteristics and outcomes in patients with COVID-19 and B-cell lymphoma treated with B-cell depleting agents
Regarding B-cell depleting therapy, there was no significant difference in total duration of TCE or RTX therapy (median [IQR], 250 [114–367] vs. 137 [89–341] days; p=0.291), but the number of cycles was significantly higher in the TCE group than that in the RTX group (median [IQR], 12 [6–14] vs. 6 [4–9]; p=0.010). Further, interval from last TCE or RTX therapy to COVID-19 diagnosis was shorter in the TCE group than in the RTX group, and a higher percentage of the TCE group had received prior therapies (85.7% vs. 55.0%, p=0.041), with 64.3% having received more than two prior therapies. Among patients who received second-line or more treatments, the detailed regimens of first-line chemotherapy vary, but there were no significant differences in chemotherapy regimens between the RTX and TCE groups (S1 Table). The proportions of cases who had undergone autologous stem-cell transplantation, chimeric antigen receptor T-cell therapy, or bendamustine therapy did not differ significantly between the TCE and RTX groups. Although lymphoma status at the time of COVID-19 did not differ significantly between the two groups, objective response rates tended to be higher in the TCE group than in the RTX group (complete response 78.6% vs. 55.0%, p=0.119; partial response 14.3% vs. 5.0%, p=0.274).
2. Clinical course and outcomes of COVID-19
Only five cases (12.5%) in the RTX group were confirmed with COVID-19 during the Delta dominant period, while all of the TCE group and 35 cases (87.5%) in the RTX group were confirmed with COVID-19 after the Omicron variant became dominant (Table 1). The number of study subjects diagnosed with COVID-19 per month showed a similar trend to the overall epidemic curve of COVID-19 in Korea (Fig. 1).
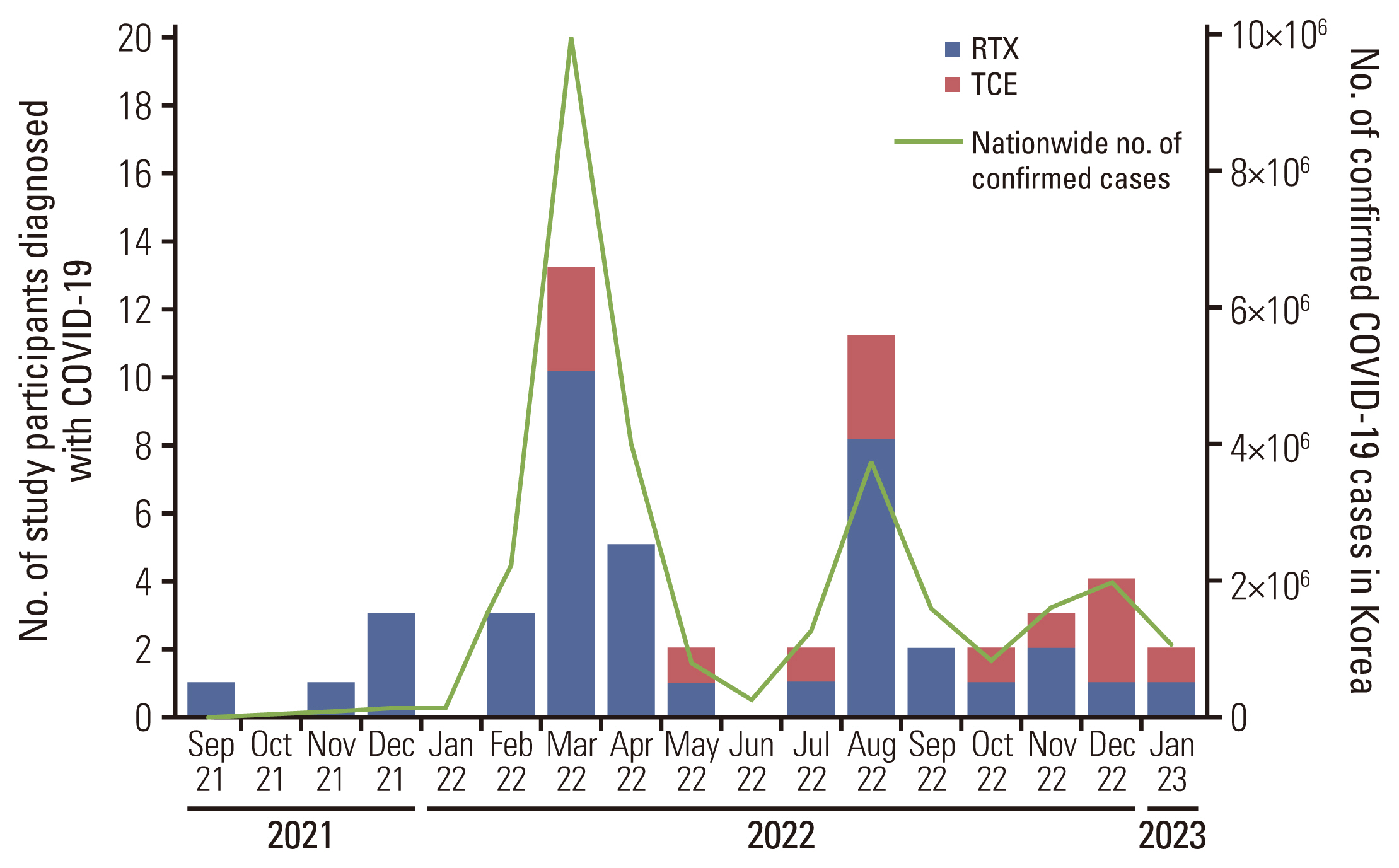
Monthly numbers of study participants receiving coronavirus disease 2019 (COVID-19) diagnosis and confirmed COVID-19 cases in Korea. RTX, rituximab; TCE, T-cell engager.
The clinical courses of COVID-19 over time since diagnosis of COVID-19 in the TCE and RTX groups is presented in Fig. 2. Except for two cases of mild COVID-19, 12 (85.7%) patients in the TCE group were treated with therapeutic remdesivir (≥ 5 days) and dexamethasone for COVID-19. In the RTX group, 21 (52.5%) were treated with therapeutic remdesivir and 14 (35.0%) were treated with dexamethasone for COVID-19.
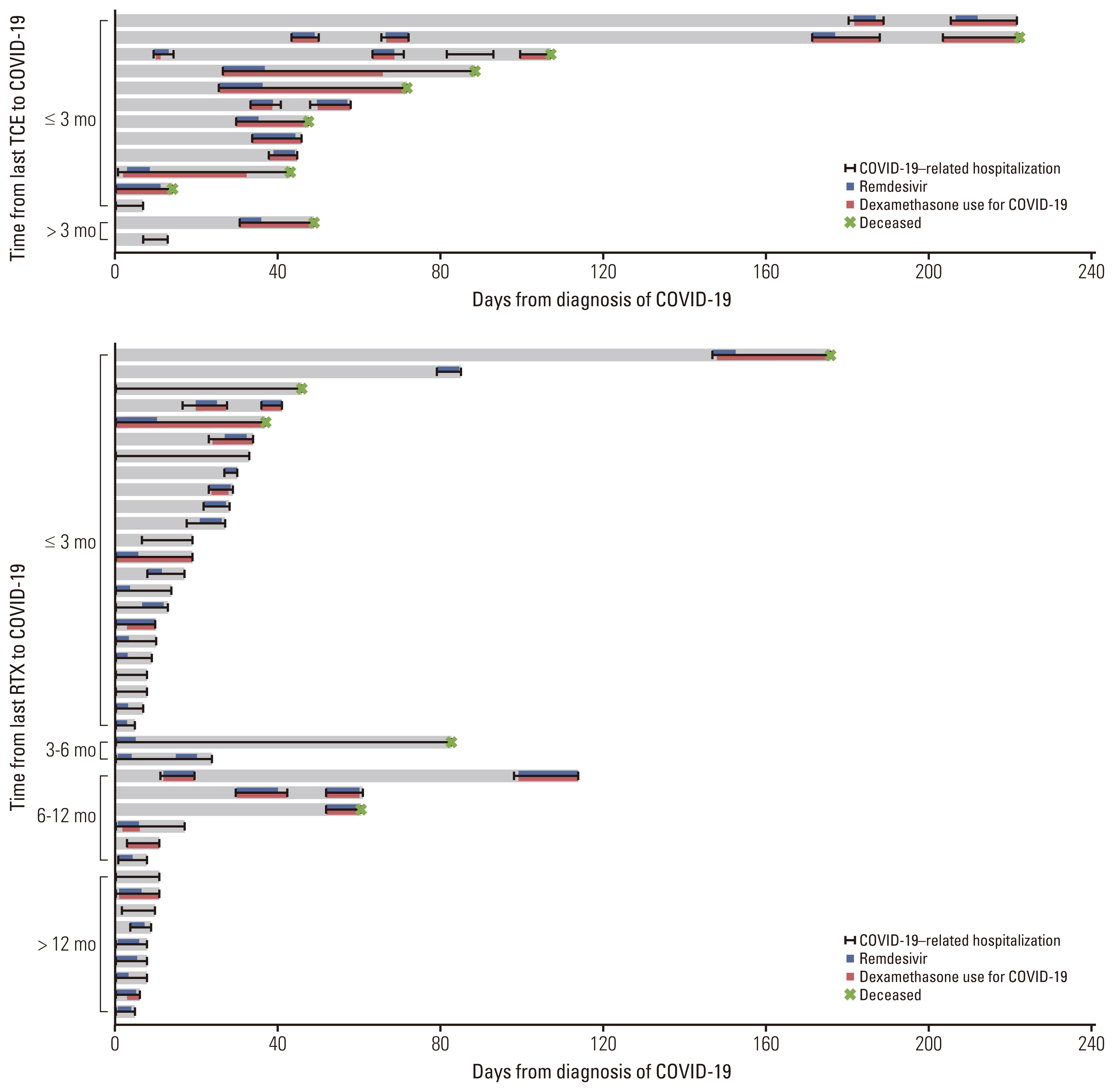
Clinical courses of patients with coronavirus disease 2019 (COVID-19) according to time from B-cell depleting therapy to COVID-19 diagnosis in the T-cell engager (TCE) and rituximab (RTX) groups.
COVID-19 severity differed significantly between the TCE and RTX groups. The proportion of patients with severe to critical COVID-19 was higher in the TCE group than in the RTX group (28.6% vs. 15.0% and 57.1% vs. 22.5%, respectively) (Table 1). The interval from COVID-19 diagnosis to discharge from COVID-19–related hospitalization was significantly longer in the TCE group than in the RTX group (median [IQR], 48 [35–93] vs. 16 [8–34] days; p=0.002). Both COVID-19–related and in-hospital mortality were also significantly higher in the TCE group than the RTX group (57.1% vs. 12.5%, p=0.002; 57.1% vs. 20.0%, p=0.016, respectively). Among patients who received second-line or more treatments, COVID-19–related morality was significantly higher in the TCE group than in the RTX group (50.0% vs. 13.6%, p=0.040) (S1 Table).
3. Risk factors for severe to critical COVID-19 and COVID-19–related mortality
Older age (odds ratio [OR], 1.08; 95% confidence interval [CI], 1.02 to 1.14; p=0.008) and TCE therapy (OR, 10.00; 95%
CI, 1.96 to 50.94; p=0.006) were associated with severe to critical COVID-19 in univariate analysis (S2 Table). Multivariable analysis identified both older age (adjusted odds ratio [aOR], 1.06; 95% CI, 1.00 to 1.13; p=0.035) and TCE therapy (aOR, 7.08; 95% CI, 1.29 to 38.76; p=0.024) as independent risk factors for severe to critical COVID-19. Subgroup analysis of patients undergoing B-cell depleting therapy within 1 year prior to COVID-19 showed that older age (aOR, 1.06; 95% CI, 1.00 to 1.13; p=0.045) and TCE therapy (aOR, 5.74; 95% CI, 1.00 to 32.85; p=0.050) were also significantly associated with severe to critical COVID-19 on multivariable analysis (S3 Table).
Univariate analysis found that older age and TCE therapy were also risk factors for COVID-19–related mortality (Table 2). On multivariable analysis, older age (aOR, 1.13; 95% CI, 1.02 to 1.26; p=0.022), TCE therapy (aOR, 8.98; 95% CI, 1.48 to 54.40; p=0.017), and prior bendamustine therapy (aOR, 7.78; 95% CI, 1.17 to 51.65; p=0.034) were significantly associated with COVID-19–related mortality. In multivariable analysis among patients receiving B-cell depleting therapy within 1 year prior to COVID-19, TCE therapy was also an independent risk factor for COVID-19–related mortality (aOR, 7.48; 95% CI, 1.17 to 47.85; p=0.034) after adjustment for age and sex (S4 Table). Subgroup analysis of patients with aggressive B-cell lymphoma also showed that TCE therapy (aOR, 8.97; 95% CI, 1.37 to 58.73; p=0.022) and prior bendamustine therapy (aOR, 8.97; 95% CI, 1.37 to 58.73; p=0.022) were significantly associated with COVID-19–related mortality (S5 Table).

Risk factors for COVID-19–related mortality in patients with B-cell lymphoma treated with B-cell depleting agents
COVID-19–related survival was significantly longer in the RTX group than in the TCE group (hazard ratio, 0.18; 95% CI, 0.05 to 0.66; log-rank p < 0.001) (Fig. 3). Overall survival in the RTX group was also significantly longer than that in the TCE group (hazard ratio, 0.36; 95% CI, 0.12 to 1.09; log-rank p=0.020) (S6 Fig.).
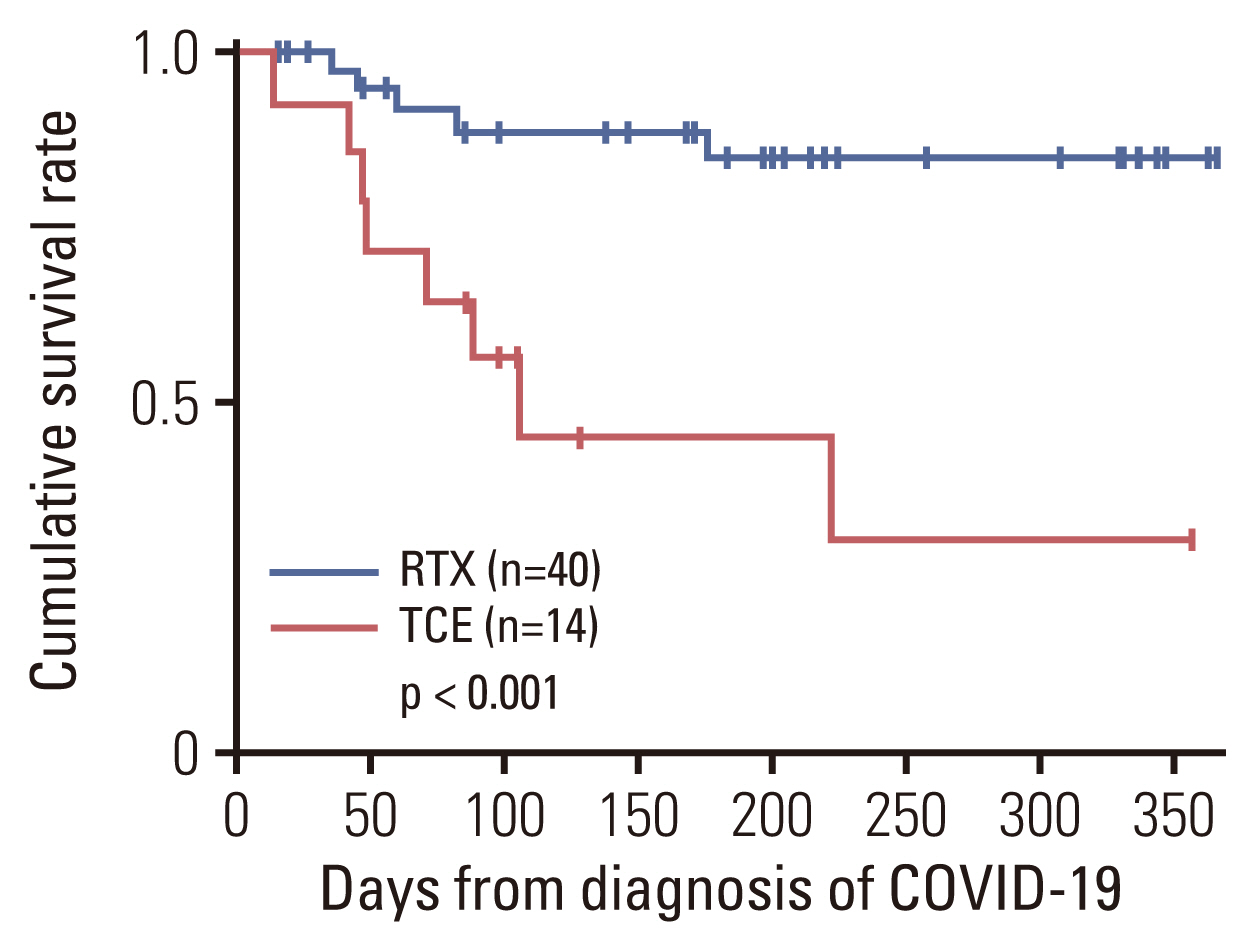
Comparison of coronavirus disease 2019 (COVID-19)–related survival between the T-cell engager (TCE) and rituximab (RTX) groups.
Discussion
To the best of our knowledge, this is the first study to compare the outcomes of COVID-19 in patients with B-cell lymphoma treated with TCE or RTX. Our data show that, despite a high complete response rate in lymphoma, patients treated with TCE had worse COVID-19–related outcomes than those treated with RTX. Multivariable analysis showed that TCE therapy was an independent risk factor for severe to critical COVID-19 and COVID-19–related mortality.
As the Omicron variant became the dominant variant of SARS-CoV-2, the risk of poor outcomes, including hospitalization and death, became lower than during the Delta dominant period [12]. Although all patients in the TCE group experienced COVID-19 in the Omicron dominant period, the outcomes of COVID-19 were grave in this group. In addition, the number of patients diagnosed with COVID-19 in this study showed a similar trend to the nationwide epidemic curve. Therefore, treatment using TCE should be considered carefully in the context of the COVID-19 epidemic situation, despite the easing of disease severity caused by more recent SARS-CoV-2 variants.
Various TCEs have been rapidly developed since the concept of specific targeting of T cells by monoclonal antibodies emerged [13]. Off-the-shelf TCEs can redirect T cells to bind to lymphoma-associated antigens on malignant B cells, to elicit T-cell–mediated cytotoxicity against B-cell lymphomas [14,15], and clinical trials suggest that TCEs show promising efficacy in patients with lymphoma [16,17]. In the present study, 78.6% of patients treated with TCEs achieved complete response, although more than 60% of patients had undergone more than two prior lines of anti-lymphoma therapy.
Several TCEs have shown manageable safety in clinical trials [18–21]; however, infections occurred as adverse events in 38% (59/155) and 20% (18/90) of patients who received TCEs in phase II clinical trials [16,17]. Although one of these trials reported COVID-19 as the most frequent infection (9%, 14/155) [16], the impact of diverse TCEs on the outcomes of COVID-19 is largely unknown. The present study clearly demonstrates that patients treated with TCEs had significantly worse outcomes of COVID-19, despite their favorable lymphoma status.
Furthermore, patients treated with TCEs usually received subsequent treatments beyond until diseases progression or the development of adverse events [21,22]. This suggests that the risk of TCEs affecting the future occurrence of atypical infections might be high, considering their mechanisms of action and the duration of treatment. Therefore, sufficient consideration is required regarding strategies to address risk of future atypical infections, and efforts should be made to improve the efficacy and safety of B-cell lymphoma treatments.
RTX is associated with hypogammaglobulinemia and an increased risk of infectious complication [23,24]. Since the global COVID-19 pandemic, several studies have reported poor outcomes of COVID-19 in patients treated with B-cell depleting therapy. A previous study of patients with COVID-19 and hematologic malignancies demonstrated that active anti-cancer therapy with monoclonal antibodies is associated with increased mortality [25]. Another study also showed that anti-CD20 therapy is a risk factor for prolonged hospitalization and death among patients with COVID-19 and non-Hodgkin lymphoma [5]. Similarly, we found that COVID-19–related mortality was relatively high among hospitalized patients treated with RTX compared with reported mortality of hospitalized patients in the general population [26].
A previous study including patients with lymphoma and a diagnosis of SARS-CoV-2 identified bendamustine exposure, active hematological disease, and comorbidity as prognostic factors for mortality [27]. Other studies have suggested that bendamustine exposure is a risk factor for patients with prolonged COVID-19 infection [28,29]. In the present study, we also showed that prior bendamustine therapy was a risk factor for COVID-19–related mortality. Bendamustine, an alkylating agent used to treat indolent and aggressive B-cell lymphomas, causes significant T-cell lymphopenia, which increases the risk of common and opportunistic infection [30], resulting in worse COVID-19–related outcomes.
Although the duration of the immunological effects of RTX on B-cell depletion and hypogammaglobulinemia is not well defined, several studies have suggested that B-cell subsets may not be fully recovered even 1 year after RTX treatment [31]. In the present study, when patients in the RTX group were classified based on time from last RTX to COVID-19 diagnosis, COVID-19–related prolonged infection or mortality were observed until 1 year after RTX therapy. Therefore, we conducted a subgroup analysis of patients treated with B-cell depleting therapy within 1 year prior to COVID-19 diagnosis, and the results were similar to those from analysis of the total patient group.
This study had several limitations. First, because it was a single-center study with a small number of hospitalized patients, the generalizability of the study findings may be limited. Nonetheless, this study included the largest cohort of patients with COVID-19 and B-cell lymphoma treated with TCE reported to date. Second, virologic characterization was not performed; however, considering the dominant variants during the study period, almost all patients treated with TCE were likely to have been infected with the Omicron variant. Third, considering the high proportion of heavily treated patients in the TCE group, it would be possible that B-cell depletion had already existed due to the prior treatment lines. Finally, the interval from last TCE or RTX therapy to COVID-19 diagnosis varied, although similar results were obtained when we excluded patients undergoing B-cell depleting therapy more than 1 year before COVID-19 diagnosis.
Our findings suggest that TCE therapy is associated with significantly worse COVID-19–related outcomes, including severe to critical COVID-19 and COVID-19–related or overall mortality, despite favorable lymphoma status, compared with RTX therapy. As the number of patients diagnosed with COVID-19 in our study was consistent with the national epidemic, we conclude that TCE therapy should be used with caution for patients with B-cell lymphoma during the COVID-19 epidemic, even when less virulent variants are dominant.
Electronic Supplementary Material
Supplementary materials are available at Cancer Research and Treatment website (https://www.e-crt.org).
Notes
Ethical Statement
This study was approved by the Institutional Review Board (IRB) of Seoul National University Hospital (IRB no. 2302-051-1402) and was conducted in accordance with the Declaration of Helsinki. Since this was a retrospective study, the need for informed consent was waived by the IRB.
Author Contributions
Conceived and designed the analysis: Kim TM, Park WB.
Collected the data: Lee CM, Choe PG, Kang CK, Jo HJ, Kim NJ, Yoon SS, Kim TM, Park WB, Oh MD.
Contributed data or analysis tools: Lee CM, Choe PG, Kang CK, Yoon SS, Kim TM, Park WB, Oh MD.
Performed the analysis: Lee CM, Choe PG, Kang CK, Kim TM, Park WB.
Wrote the paper: Lee CM, Choe PG, Kim TM, Park WB, Oh MD.
Conflicts of Interest
Dr Nam Joong Kim reported receiving research grant from GC Biopharma. Dr Sung-Soo Yoon reported receiving research grants from Roche-Genentech, Yuhan Pharma, JW Pharmaceutical Corporation, Kyowa Hakko Kirin, and Chong Kun Dang Pharmaceutical Corp; receiving honoraria from Novartis, Celgene, and Janssen; and participating in data safety monitoring board or advisory board meetings for Amgen, Antengene, Novartis, Janssen, Regeneron, Takeda. Dr Tae Min Kim reported receiving research grant from AstraZeneca-KHIDI; and participating in advisory board meetings or consulting roles for AstraZeneca/MedImmune, Boryung, Hanmi, IMBDx, Novartis, Takeda, Regeneron, Roche/Genentech, Samsung Bioepis, and Yuhan. Dr Wan Beom Park reported receiving research grant from Yuhan, Gilead, Metacura, QuantaMatrix, and Pfizer. Dr Myoung-don Oh reported receiving research grant from Daewoong Pharmaceutical, MSD, and SK Bioscience. No other disclosures were reported.
Acknowledgments
This study was supported by the Bio & Medical Technology Development Program of the National Research Foundation (NRF) and funded by the Korean government (MSIT) (grant number, 2021M3A9I2080498).