Colonoscopic Screening and Risk of All-Cause and Colorectal Cancer Mortality in Young and Older Individuals
Article information

Abstract
Purpose
The incidence of early-onset colorectal cancer (CRC) and associated mortality have been increasing. However, the potential benefits of CRC screening are largely unknown in young individuals. We aimed to evaluate the effect of CRC screening with colonoscopy on all-cause and CRC mortality among young (aged < 45 years) and older (aged ≥ 45 years) individuals.
Materials and Methods
This cohort study included 528,046 Korean adults free of cancer at baseline who underwent a comprehensive health examination. The colonoscopic screening group was defined as those who reported undergoing colonoscopy for CRC screening. Mortality follow-up until December 31, 2019 was ascertained based on nationwide death certificate data from the Korea National Statistical Office.
Results
Colonoscopic screening was associated with a lower risk of all-cause mortality in both young and older individuals. Multivariable-adjusted time-dependent hazard ratios (95% confidence intervals) for all-cause mortality comparing ever-to never-screening were 0.86 (0.75–0.99) for young individuals and 0.71 (0.65–0.78) for older individuals. Colonoscopic screenings were also associated with a reduced risk of CRC mortality without significant interaction by age, although this association was significant only among participants aged ≥ 45 years, with corresponding time-dependent hazard ratios of 0.47 (0.15–1.44) for young individuals and 0.52 (0.31–0.87) for those aged ≥ 45 years.
Conclusion
Colonoscopic CRC screening decreased all-cause mortality among both young and older individuals, while significantly decreased CRC mortality was observed only in those aged ≥ 45 years. Screening initiation at an earlier age warrants more rigorous confirmatory studies.
Introduction
Colorectal cancer (CRC) is a common gastrointestinal cancer, and is the third leading cause of cancer deaths worldwide [1]. In Korea, CRC was the third most common cancer (excluding thyroid cancer) in 2018 and has been increasing steadily [2]. Generally, the risk of CRC increases with age; however, its incidence and mortality have been increasing worldwide in young individuals aged < 50 years [3–5].
CRC is one of the most preventable and treatable cancers with early detection [6–8]. The US Preventive Services Task Force (USPSTF) guideline has recently been updated with the recommendation of screening for CRC starting at the age of 45 years [9,10]. While accumulating evidence suggests that the incidence of early-onset CRC and associated mortality have been increasing at an alarming rate [11], data on the potential effect of CRC screening in individuals younger aged < 45 years are scarce since younger individuals are not usually recommended screening for CRC.
Most previous studies reported the effect of screening interventions that mainly included a fecal occult blood test (FOBT) [12] or sigmoidoscopy [7]. However, there have been few studies that focused on the effect of colonoscopic screening [13] even though colonoscopic screening, among CRC screening strategies, may result in a larger reduction in CRC incidence and mortality compared to sigmoidoscopy and an annual FOBT [14]. In addition, some studies on CRC screening have demonstrated a significant decrease in CRC incidence and mortality [15] but with inconsistent results or even increases in non-CRC and all-cause mortality [16–18]. Furthermore, the colonoscopic screening effect in individuals aged < 45 years is largely unknown. Thus, we aimed to evaluate the effect of colonoscopic screening for CRC with an analysis of all-cause and CRC mortality according to age group (< 45 years and ≥ 45 years, with 45 years being the initiation age of average-risk CRC screening described in the recent USPSTF guidelines for CRC screening).
Materials and Methods
1. Study population
The Kangbuk Samsung Health Study was a cohort study of Korean men and women aged 18 years or older who underwent an annual or biennial routine health check-up at one of the Kangbuk Samsung Hospital Total Healthcare Centers in Seoul or Suwon, South Korea [19]. In South Korea, the Industrial Safety and Health Law requires annual or biennial health screening examinations of all employees, which are offered free of charge. The present cohort study was restricted to participants who underwent health examinations between January 1, 2007 and December 31, 2017 (n=548,460). We excluded 20,414 participants (3.7%) who met one or more of the following criteria at baseline: unknown vital status due to an invalid identifier (n=3), missing data on colonoscopic screening (n=138), missing data on previous history of cancer (n=11,104), and having a positive FOBT at baseline (n=9,406). Ultimately, 528,046 participants were eligible for this study (Fig. 1).
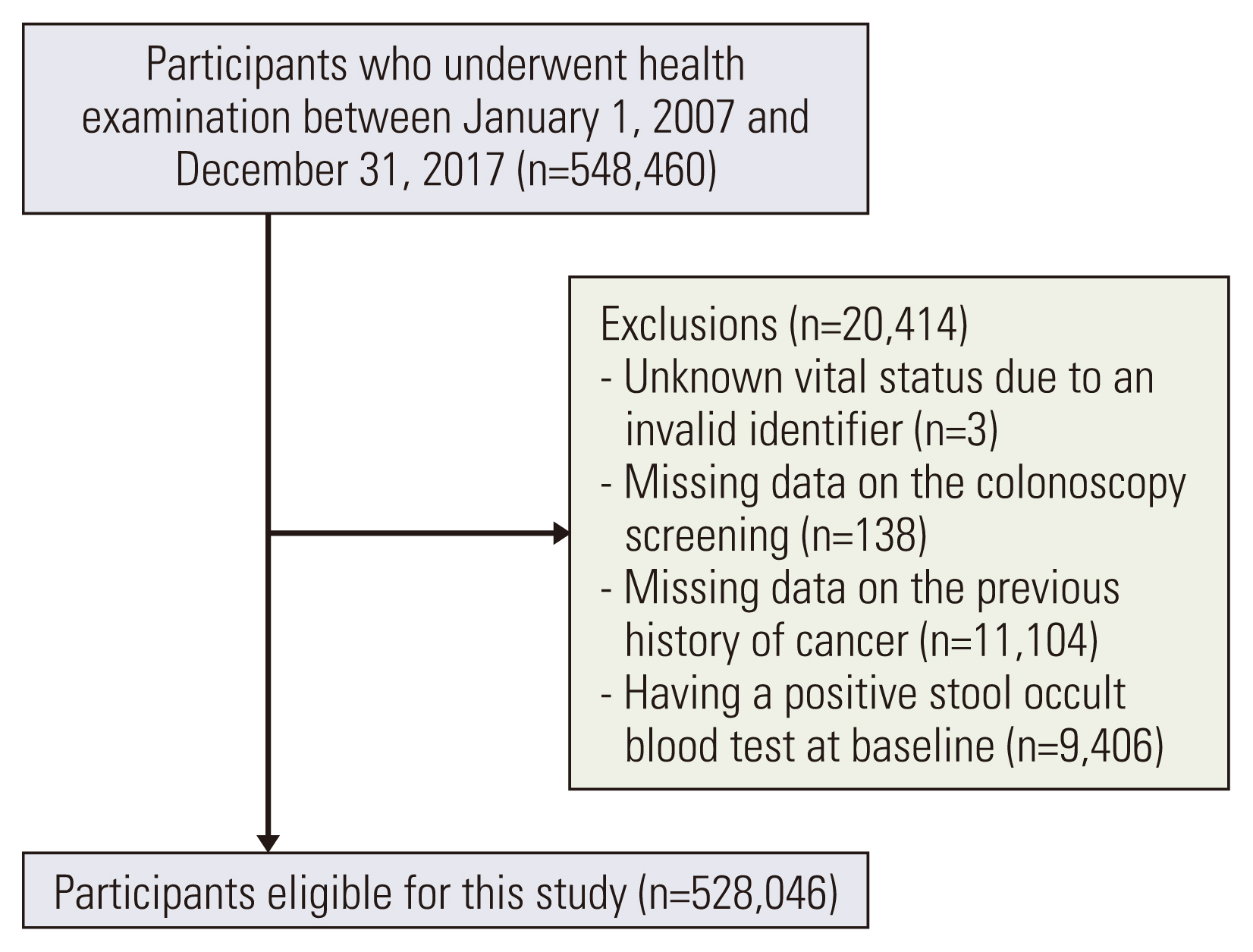
Flow chart of study participants.
2. Data collection
Demographic characteristics, behavioral factors, and medical histories were collected using a standardized, self-administered questionnaire. Current smokers were defined as individuals who had a lifetime history of smoking 100 or more cigarettes and were active smokers at the time of examination. The average alcohol intake was categorized as none, < 20 g/day, and ≥ 20 g/day [20]; regular exercise was defined as performance of moderate or vigorous physical activity ≥ 3 times/wk.
Anthropometric parameters and sitting blood pressure were measured by trained nurses. Body mass index was calculated as (weight in kg)/(height in meters)2. Obesity was defined as a body mass index ≥ 25 kg/m2 using the proposed cutoff for a diagnosis of obesity in Asians [21]. Hypertension was defined as blood pressure ≥ 140/90 mmHg or the use of antihypertensive medication. Fasting blood tests included serum levels of glucose, insulin, total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides, liver enzymes, and high-sensitivity C-reactive protein. Insulin resistance was assessed using the homeostatic model assessment of insulin resistance equation as follows: fasting blood insulin (μU/mL)×fasting blood glucose (mmol/L)/22.5. Diabetes mellitus was defined as a fasting serum glucose level ≥ 126 mg/dL, hemoglobin A1c ≥ 6.5%, or current use of anti-diabetic medication. The Laboratory Medicine Department at Kangbuk Samsung Hospital in Seoul, Korea, has been accredited by the Korean Society of Laboratory Medicine, the Korean Association of Quality Assurance for Clinical Laboratories, and the College of American Pathologists Survey Proficiency Testing.
3. Definition of colonoscopic screening for CRC
We defined the ever-colonoscopic-screening group as individuals who underwent colonoscopic screening for CRC when visiting the healthcare center for routine or age-related screenings. To classify participants who received colonoscopic screening in other healthcare centers, we asked participants whether they have received colonoscopy in their lifetime. The never-screening group was defined as individuals who had never undergone colonoscopy at the time of examination. Participants were included in the never-screening group until the first time they reported receiving a colonoscopic screening or colonoscopy at a healthcare center. They were included in the ever-screening group after receiving colonoscopy at the follow-up visit. The ever-screening group was defined as the group that had undergone colonoscopy and was further categorized into three groups: screening within 5 years, more than 5 years, and unknown.
4. Ascertainment of all-cause and CRC mortality
Mortality follow-up until the end of 2019 was based on nationwide death certificate data from the Korea National Statistical Office. The cause of death was determined based on the underlying cause listed on each death certificate, which was classified according to the International Classification of Diseases and Related Health Problems 10th revision (ICD-10). The concordance between the cause of death on the death certificate and the patient diagnosis in the medical utilization data was 91.9% across all causes of death and 94.9% for cancer deaths [22,23]. CRC mortality was defined as the ICD-10 codes for CRCs (C18–20).
5. Statistical analysis
The baseline characteristics of the study participants were presented according to colonoscopic screening. All data were presented as means (95% confidence interval [CI]) or proportions adjusted for age and sex (95% CI), as appropriate. The primary outcomes were all-cause and CRC-specific mortality. Each participant was followed until December 31, 2019 or the time of death, whichever came first. As the baseline characteristics of the study participants differed according to colonoscopic screening, we used inverse probability weights to compensate for any imbalance in the study groups. In addition, we evaluated the effect of CRC screening with colonoscopy after excluding participants who underwent FOBT during follow-up. Hazard ratios (HRs) and 95% CIs for all-cause mortality and CRC mortality were estimated using Cox proportional hazard regression analyses with age as the timescale. To evaluate the effect of colonoscopic screening, we classified individuals into two groups (< 45 years and ≥ 45 years) according to the USPSTF recommendation for initiating CRC screening at the age of 45 [10]. Models were initially adjusted for age (timescale) and sex, and then further adjusted for year of screening exam, study center, obesity, smoking status, regular exercise, alcohol intake, educational level, family history of cancer, hyperlipidemia medication, history of diabetes, history of hypertension, and history of cardiovascular disease. We conducted time-dependent analyses in which changes in colonoscopic screenings and covariates during follow-up were updated in the models. Likelihood ratio tests were used to test interactions by age (age < 45 vs. age ≥ 45), comparing models with and without multiplicative interaction terms. Statistical analyses were performed using STATA ver. 16.0 (StataCorp LP, College Station, TX). Statistical significance was established at a two-tailed p-value of < 0.05.
6. Data availability
The data are not publicly shared because we do not have permission from the Institutional Review Board to distribute the data. The analytic methods are available from the corresponding authors upon reasonable request.
Results
1. Baseline characteristics of the study participants
The baseline characteristics of the study participants are shown in Table 1, which presents the mean values and proportions according to colonoscopic screening after adjusting for age and sex. Total 528,046 Korean adults (median age, 37.2 years) were followed up for a median of 8.0 years (interquartile range, 5.0 to 11.1 years). Among total participants, 357,325 (67.7%) were included in the never-screening group and 170,721 (32.3%) in the ever-screening group. The mean age was 43.5 years in the ever-screening group and 38.1 years in the never-screening group. The ever-screening group had a higher proportion of men (61.6% vs. 48.3%), lower smoking prevalence (21.0% vs. 22.8%), higher alcohol intake (22.8% vs. 18.0%), and more frequent family history of cancer (27.9% vs. 22.8%) compared with the never-screening group.

2. All-cause mortality by colonoscopic screening
Table 2 shows the number of deaths, mortality rates, and HRs for all-cause mortality according to colonoscopic screening for CRC. A total of 6,790 deaths occurred in 12,775,275 person-years among the never-screening group (all-cause mortality rate, 53.1 per 105 person-years) and 3,257 deaths in 4,034,205 person-years among the ever-screening group (all-cause mortality rate, 80.7 per 105 person-years). Among the participants aged < 45 years, the all-cause mortality rate was 32.6 per 105 person-years in the never-screening group and 37.4 per 105 person-years in the ever-screening group. Among the participants aged ≥ 45 years, the all-cause mortality rate was 210.1 per 105 person-years in the never-screening group and 188.0 per 105 person-years among the ever-screening group. Using the time-dependent variables in the Cox proportional hazard model, the HRs for all-cause mortality of all participants were significantly decreased in the ever-screening group (HR, 0.67; 95% CI, 0.62 to 0.73). The ever-screening group showed a lower risk of all-cause mortality among participants aged ≥ 45 (HR, 0.71; 95% CI, 0.65 to 0.78) and < 45 years (HR, 0.86; 95% CI, 0.75 to 0.99). Regarding all-cause mortality according to screening period, the HRs (95% CI) for all-cause mortality of the total participants in the ever-screening group within 5 years and over 5 years were 0.67 (0.62–0.73) and 0.63 (0.53–0.77), respectively, compared with the never-screening group (S1 Table). In addition, after excluding participants with a positive FOBT during follow-up, colonoscopic screening still reduced all-cause mortality among all participants and aged ≥ 45 participants (S2 Table).

All-cause mortality by colonoscopic screening
3. CRC mortality by colonoscopic screening
Table 3 shows the number of CRC deaths and HRs for CRC mortality according to colonoscopic screening. The HRs for CRC mortality were significantly decreased in the ever-screening group overall (HR, 0.50; 95% CI, 0.31 to 0.80) and among participants aged ≥ 45 years (HR, 0.52; 95% CI, 0.31 to 0.87) in the model using time-dependent variables. The risk for CRC mortality was not decreased in the ever-screening group among participants aged < 45 years (HR, 0.47; 95% CI, 0.15 to 1.44). Regarding CRC mortality according to the screening period, the HRs (95% CI) for CRC mortality of all participants was 0.53 (0.32–0.86) in the ever-screening group within 5 years (S1 Table). After excluding participants with a positive FOBT during follow-up, colonoscopic screening tended to decrease CRC mortality among all participants (HR, 0.68; 95% CI, 0.36 to 1.30) and participants aged ≥ 45 years (HR, 0.59; 95% CI, 0.33 to 1.06), although neither reached statistical significance (S2 Table).

Colorectal cancer mortality by colonoscopic screening
Discussion
The present study demonstrated that colonoscopic screening was associated with a decreased risk of both CRC mortality and all-cause mortality in a large cohort of Korean men and women, especially among those aged ≥ 45 years. For individuals aged < 45 years, colonoscopic screening significantly decreased all-cause mortality but not CRC mortality. Our findings suggest that CRC screening with colonoscopy is beneficial in adults aged ≥ 45 years, with a significant reduction in both all-cause and CRC mortality.
Although a recent study with a long-term follow-up period reported an all-cause mortality reduction associated with biennial FOBT screening [17], previous studies and meta-analyses have mostly reported that CRC screening is associated with a reduced risk of CRC mortality, but not all-cause mortality [7,12,15]. If CRC screening decreases CRC mortality but does not reduce all-cause mortality because of its complications, it might not have a substantial health benefit among the screened population [16]. Contrary to several previous studies [7,12,15], our results showed that CRC screening with colonoscopy reduced both all-cause mortality and CRC mortality. There are several possible reasons for our results. First, among all CRC screening interventions, colonoscopy may have a larger health benefit compared to sigmoidoscopy and an annual FOBT [14]. We supposed that individuals at an elevated risk of CRC were able to have existing adenomas or precancerous polyps removed through colonoscopy, which may have led to favorable outcomes [6]. In addition, because we performed time-dependent analyses considering colonoscopic screening at follow-up, we were able to obtain more reliable results compared to studies that only considered baseline screening status. Variables analyzed using the time-fixed approach may lead to biased results and underestimation of the effect size of CRC screening because it classifies screened individuals only at baseline and does not consider that never-screened individuals at baseline may have received colonoscopy during follow-up. In addition, most previous reports suggest that individuals who receive positive results on a CRC screening are likely to modify their lifestyles, which, in turn, helps reduce the risk of all-cause mortality [24,25]. Furthermore, given that our study population mainly comprised younger adults in their mid-40s with relatively higher socioeconomic statuses, it is probable that they had better access to medical care as compared to the general population [26,27]. Another possible explanation is a lower chance of fatal adverse events or unexpected harm caused by screening in younger individuals, such as post-polypectomy bleeding or perforation, which can be especially fatal in older populations [28–30].
In our study, the ever-screening group participants aged < 45 years had significantly reduced all-cause mortality but not CRC mortality compared to the never-screening group. This may be due to the low number of CRC incidences and deaths occurring at a young age [31]. In addition, people at a higher risk of CRC would be more prone to receive CRC screening than the low-risk group [32], and such a tendency would be more pronounced in younger individuals as they are not likely to receive CRC screening unless they become symptomatic [33]. Given our observation that colonoscopy was indeed effective in reducing all-cause mortality, future studies are necessary to clarify the association between CRC screening and CRC mortality and the preventive value of the screening in at-risk individuals aged < 45 years.
A previous study reported that once-only sigmoidoscopy for CRC screening was associated with a reduced risk of CRC death [7]. Likewise, lifetime once-only colonoscopy may also have a protective effect on CRC mortality, possibly because it can help remove adenomas or precancerous polyps [6]. However, we found no differences in the risk according to colonoscopic screening period in our study. Considering that the recommended interval for screening is 10 years for the general population [10,34], the follow-up period of our study may not have been sufficient for screening interval analyses, which partly explains the discrepancy between our findings and those of previous reports. Further longitudinal studies could elucidate the effects of CRC screening intervals on CRC and all-cause mortality.
Our study has several limitations. First, we investigated colonoscopic screening status using either data from colonoscopic examinations or a self-reported questionnaire conducted at health check-up centers of Kangbuk Hospital. According to a previous meta-analysis, the accuracy of CRC screening history based on self-reports showed a high specificity and moderate sensitivity [35]. There were individuals who had undergone colonoscopy at other medical centers during the follow-up, who may have been misclassified to the non-screening group. Second, our study participants were predominantly healthy workers with a higher socioeconomic status compared to the general Korean population, thereby limiting the generalizability of our findings. Nonetheless, because our participants were relatively healthier than the general population, the mortality reduction of colonoscopic screening for CRC could have been underestimated. Third, as we did not have access to the data on colonoscopic polypectomy and histology, we were not able to accurately measure the intervention effect of the colonoscopic screening. Despite these limitations, our study has considerable strengths, including the large sample size, standardized questionnaires, and time-varying assessment of colonoscopic screening using a reasonable analysis method.
In conclusion, CRC screening using colonoscopy reduced both all-cause and CRC mortality, especially among individuals aged ≥ 45 years, which supports the updated USPSTF recommendation. In the younger age group, CRC screening was associated with a reduction in all-cause mortality, but not CRC mortality. Further studies are necessary to determine the preventive value of CRC screening in at-risk individuals aged < 45 years.
Electronic Supplementary Material
Supplementary materials are available at Cancer Research and Treatment website (https://www.e-crt.org).
Notes
Ethical Statement
This study was approved by the Institutional Review Board of Kangbuk Samsung Hospital, which waived the requirement for informed consent due to the use of anonymized data routinely collected as part of a health check-up program and already linked to mortality data from the Korea National Statistical Office (IRB No. 2011-01-030-005 for the general Kangbuk Samsung Health Study protocol and 2021-10-032 for the present study).
Author Contributions
Conceived and designed the analysis: Lee JA, Chang Y, Ryu S.
Acquisition, analysis, or interpretation of data: Lee JA, Chang Y, Kim Y, Park DI, Park SK, Park HY, Koh J, Lee SJ, Ryu S.
Wrote the paper: Lee JA, Chang Y.
Critical revision of the manuscript for important intellectual content: Lee JA, Chang Y, Kim Y, Park DI, Park SK, Park HY, Koh J, Lee SJ, Ryu S.
Statistical analysis: Chang Y, Ryu S.
Obtained funding: Chang Y, Ryu S.
Supervision: Chang Y, Ryu S.
Conflicts of Interest
Conflict of interest relevant to this article was not reported.
Acknowledgments
This study was supported by the SKKU Excellence in Research Award Research Fund, Sungkyunkwan University, 2020. The funding sources had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and the decision to submit the manuscript for publication.