Treating Oligometastses, Prelude or Just Hassles of Systemic Treatment
Article information

The concept of “oligometastatic disease” was first proposed by Hellman and Weichselbaum as a distinct clinical state between locally confined and systemically metastasized disease in 1995 [1]. The thought that treating metastasis-directed therapy (MDT) for oligometastatic disease has the potential for cure or long-term disease control has been very appealing like two old hypotheses of Paget’s “seed and soil” and Ewing’s “mechanical mechanism” [2–4]. The hypotheses could explain clinical situations that resection of limited metastatic tumors in the brain, lung or liver resulted in very good outcomes and even cure. Since the concept of oligometastatic disease has become more generally accepted, MDT, such as surgical resection or radiotherapy, is often offered with curative rather than palliative intent. In addition, owing to rapid advancement in technologies and radiotherapy techniques, stereotactic body radiotherapy (SBRT) has become more affordable recently. The number of publications of MDT has skyrocketed and more data has accumulated [5]. But, there is still some hesitancy or reluctance due to the lack of confirmative results by phase III studies on the efficacy or (cost-) effectiveness. What is worse, a disappointing result was recently reported from NRG-BR002 study which is one of the ongoing phase III studies evaluating the role of MDT when added to systemic therapy for predefined oligometastatic disease (Table 1) [6]. Based on NRG-BR002 study, the addition of MDT did not translate into better survival outcomes, suggesting that it might be of no or little use in the context of currently effective systemic treatment. We cannot draw a conclusion, however, that MDT plays no or little role in all tumor types or all clinical settings. There are many tumor types with different tumor biology, and furthermore, oligometastatic disease should encompass quite diverse clinical situations, such as de novo oligometastasis, oligo-recurrence, oligo-progression, and oligo-persistence [7]. In this regard, a meta-analysis reported by Rim et al is very helpful to gain an insight and clinical guidance in treating oligometastatic disease [8]. Nevertheless, one question occurs inevitably to us. What if systemic therapy improves enough to eradicate cancer cells or metastatic disease? This is actually happening! Advance and repeating success of immune-oncology has rapidly changed the landscape of systemic treatment so that the indications have expanded rapidly from clinically over metastatic disease to micrometastatic disease in adjuvant and neo-adjuvant settings with improving the chances for cure. Therefore, subsequent research following Rim et al.’s meta-analysis is needed to focus on MDT in the context of systemic therapy in very diverse clinical situations and could define its role more specifically. The devil is in the detail, and God is also in the detail likewise.
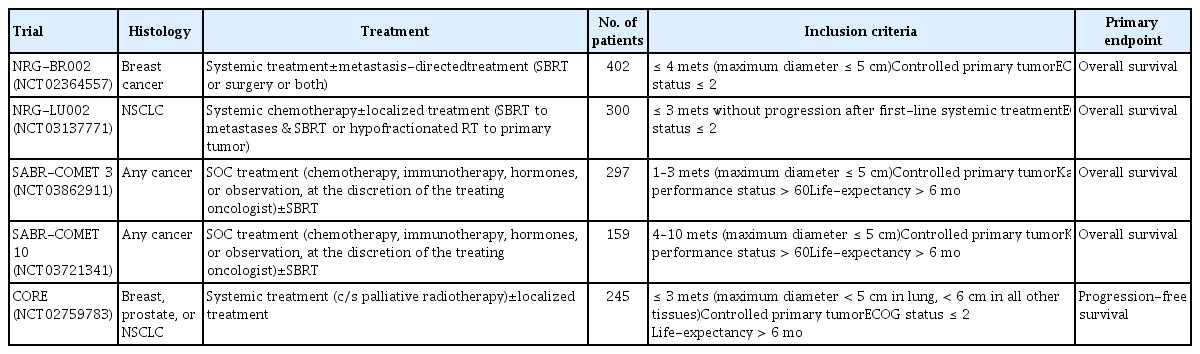
Currently ongoing prospective randomized phase III studies for oligometastatic disease
Unfortunately, Rim et al.’s meta-analysis did not deal with biological aspects of oligometastatic disease. Basically, the biologic concept of “oligometastatic disease” is challengeable like that “seed and soil” or “mechanical mechanism” hypothesis was challenged by others such as “tumor self-seeding” hypothesis [9,10]. There is cumulative evidence that both mechanical mechanism, such as hemodynamic and anatomical factors, and fruitful soil play complementary roles in tumor dissemination. There is also contradictory evidence, however, that intrinsic metastatic traits of seeds or cancer cells play a critical role. Research for identifying the biomarkers representing seed, soil or mechanical factors will be needed. On the other hand, “oligometastatic disease” might be a certain point in the temporospatial continuum of cancer rather than the binary or all-or-nothing state, leading to the postulation that a low-volume metastatic disease may still be curable with definitive MDT. Research for defining “oligometastatic disease” or “oligometastatic state” could be more important than that for identifying the biomarkers representing each factor. In this regard, the development of analyzing technology of circulating tumor cells or tumor DNA is noteworthy as a good method for defining the oligometastatic disease or state. Up to a certain point, we can give curative MDT without additional or concurrent systemic therapy. The point might change according to the state and the nature of tumors but MDT can be played like a prelude, which is played as an introduction to a larger musical piece, but also is played as a brief and self-contained one.