Clinical Experience of Male Primary Choriocarcinoma at the Samsung Medical Center
Article information
Abstract
Purpose
The objective of this study was to describe and analyze the clinicopathological features of primary choriocarcinoma (PCC) observed in male patients treated at the Samsung Medical Center between 1996 and 2020.
Materials and Methods
We reviewed the clinical records of 14 male patients with PCC retrospectively to assess their demographic, histological, and clinical characteristics at the time of diagnosis as well as identify the treatment outcomes.
Results
The median age of the patients was 33 years. The primary tumor site was the testicles in seven cases (50%), the mediastinum in six cases (43%), and the brain in one case (7%). The most common metastatic site was the lungs (79%), followed by the brain (43%). All patients with PCC received cytotoxic chemotherapy. Twelve patients had records of their response to cytotoxic chemotherapy; of these 12 patients, eight (8/12, 67%) achieved an objective response, and four (4/12, 33%) achieved stable disease response as the best response during chemotherapy.
Conclusion
It is known that most male PCC patients eventually develop resistance to cytotoxic chemotherapy and die. Factors such as poor response to chemotherapy, high disease burden, brain metastasis, and hemoptysis at the time of diagnosis are associated with shorter survival time in male PCC patients. Programmed death-1/programmed death-ligand 1 blockade therapy can be a salvage treatment for chemotherapy-resistant male PCC patients.
Introduction
Testicular germ cell tumors (TGCTs) are the most common solid tumors in young men between the ages of 20 and 34 [1]. Although TGCTs most commonly arise in the testicles, occasionally they develop in extragonadal sites without the presence of a primary tumor in the testicles. Extragonadal TGCTs mainly develop in midline locations of the body, such as the anterior mediastinum, retroperitoneum, and pineal gland [2]. TGCTs are divided into two major histological types: pure classic seminoma and non-seminomatous germ cell tumors (NSGCTs) [3]. NSGCTs can be of four subtypes, embryonal carcinoma, yolk sac tumor, teratoma, and choriocarcinoma, and can present a mix of seminomatous and nonseminomatous components. Seminoma often demonstrates indolent behavior, while NSGCTs tend to occur at a younger age and confer higher mortality.
Choriocarcinoma is a rare cancer composed of cytotrophoblasts, intermediate trophoblasts, and syncytiotrophoblast cells [4]. In embryology, these trophoblast cells are known to contribute to the implantation and subsequent placental development and secrete human chorionic gonadotropin (hCG) to promote the maintenance of the corpus luteum. Therefore, hCG is used as a tumor marker of choriocarcinoma. Choriocarcinoma is classified as gestational or nongestational [5]. Gestational choriocarcinoma refers to choriocarcinoma originating from the trophoblast of any type of gestational event, such as hydatidiform mole, spontaneous abortion, and normal pregnancy. Nongestational choriocarcinoma refers to choriocarcinoma that does not arise from a pregnancy event [6]. Nongestational choriocarcinoma, also called primary choriocarcinoma (PCC), can occur in men, but it is extremely rare [7].
In men, choriocarcinoma is the subtype of NSGCTs with the worst prognosis that presents with high levels of hCG, often widespread metastatic disease, and rapid progression of disease [8]. Moreover, some high-risk patients with very advanced choriocarcinoma develop choriocarcinoma syndrome, which is associated with hemorrhage from the metastatic sites, especially lungs, and has very high mortality rates [4]. To date, the mechanism of male PCC development is not well understood, but the following three hypotheses have been suggested [7]: (1) PCC may arise from retained primordial germ cells that migrate abnormally during embryogenesis; (2) PCC may be a testicular choriocarcinoma metastasis that regressed spontaneously or not; and (3) PCC may initially develop as a nontrophoblastic neoplasm and then transform into a choriocarcinoma.
Male PCC is extremely rare, and only few case reports have been published. The clinical features and prognostic factors of male PCC are not well known. Recently, Jiang et al. [7] analyzed data from 113 male patients with PCC and described their clinicopathological features. In this retrospective study, we describe and analyze the clinicopathological features of 14 cases of male PCC, over the age of 20, diagnosed and treated at the Samsung Medical Center (SMC) between 1996 and 2020.
Materials and Methods
1. Study population and design
A total of 20 male patients with PCC were treated at SMC between 1996 and 2020. Five patients were under the age of 20, and one was diagnosed at another hospital. We excluded these six patients and, finally, 14 male patients with PCC, all aged over 20 years, were included in this retrospective study. All patients were diagnosed on a pathological examination. The medical records of the patients were reviewed, and information on patient death was acquired from census data. The demographic, histological, and clinical characteristics of the patients at diagnosis were described and used for the analysis. Treatment and clinical outcomes of the patients were obtained from medical records.
2. Statistical analysis
Statistical analysis was performed to identify the clinical factors affecting overall survival (OS). Briefly, patients were divided into two groups according to clinical characteristics that were expected to influence OS. The OS for each group was estimated using the Kaplan-Meier method. The difference in OS between the two groups was evaluated with the log-rank test. The estimated median OS was used as a representative value for the survival rate. Additionally, the chi-square test was used to confirm association between two different clinical factors used to divide patients into two groups (data not shown). Among many factors, only the association between histologic finding and hemoptysis at the time of diagnosis was statistically significant (p=0.031). All statistical analyses were performed using the SPSS ver. 22 statistical software (IBM Corp., Armonk, NY). Statistical significance was set at p < 0.05.
Results
1. Demographic, histological, and clinical characteristics of 14 male patients with PCC at the time of diagnosis
The demographic, histological, and clinical characteristics of 14 male patients with PCC at the time of diagnosis are presented in Table 1. The median age was 33 years (range, 23 to 62 years), and most of the patients were between 20 and 40 years old. Histologically, nine cases (64%) were pure choriocarcinoma, and five cases (36%) were mixed germ cell tumors (MGCTs) including choriocarcinoma and seminoma, germinoma, teratoma, endodermal sinus tumor, and embryonal carcinoma. hCG levels were elevated in all cases, and lactate dehydrogenase levels were elevated in all examined patients (not shown). α-Fetoprotein (AFP) was elevated only in some cases (6/14, 43%).

Demographic, histological, and clinical characteristics of 14 male patients with primary choriocarcinoma
The primary tumor site was the testicles in seven cases (50%), mediastinum in six cases (43%), and brain in one case (7%). In a study by Jiang et al., the testicles were the most common primary tumor site (36.2%), and mediastinal PCC only accounted for 11% of the 113 PCC male patients assessed [7]. Due to the small number of cases in our study, caution is needed in interpreting these results. As previously mentioned, there is a hypothesis that PCC might be a testicular choriocarcinoma metastasis that has either spontaneously regressed or not. Among our cases, one patient described that right testicular swelling occurred about a year ago and had improved at the time of diagnosis. However, testicular sonography revealed that a small testicular mass still existed in his right testis. On the other hand, there was no history of testicular swelling in the other patients with extragonadal PCC.
Except for one patient with brain PCC, all other patients had metastatic diseases. The most common metastatic site was the lungs (11/14, 79%), followed by the brain (6/14, 43%), liver (4/14, 29%), and retroperitoneum (4/14, 29%). Initial symptoms varied and were related to the primary and metastatic sites of tumors. Hemoptysis, which is related to the choriocarcinoma syndrome, was present only in some patients with lung metastasis, at the time of diagnosis (6/11, 55%). Interestingly, all patients with hemoptysis at the time of diagnosis had pure choriocarcinoma histology.
2. Treatment and clinical outcomes of 14 male patients with PCC
The treatment and clinical outcomes of the patients with PCC are also presented in Table 2. Of the seven patients with testicular PCC, four (4/7, 57%) underwent orchiectomy. In addition, one patient with brain tumor underwent surgical tumor removal, and one patient with small bowel tumor underwent small bowel resection because of excessive bleeding. Excluding these six patients, the remaining patients only underwent biopsy without surgical tumor removal.
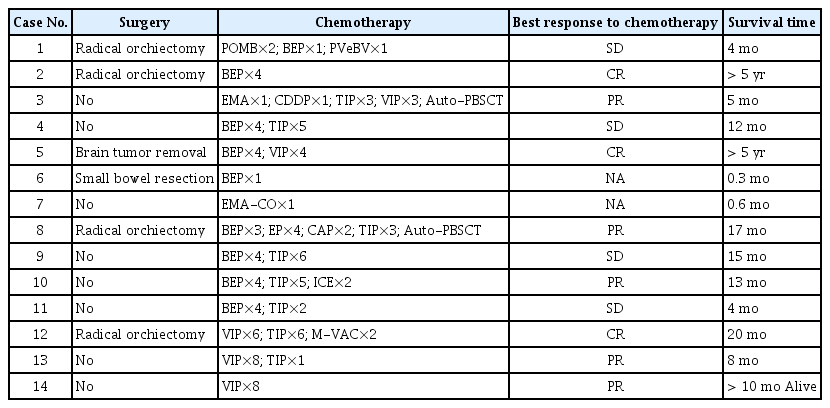
Treatment and clinical outcomes of 14 male patients with primary choriocarcinoma
All patients with PCC received cytotoxic chemotherapy. Various chemotherapeutic regimens were used, such as POMB (cisplatin, vincristine, methotrexate, bleomycin), EMA-CO (etoposide, methotrexate, actinomycin D, cyclophosphamide, vincristine), BEP (bleomycin, etoposide, cisplatin), VIP (etoposide, ifosfamide, cisplatin), and TIP (paclitaxel, ifosfamide, cisplatin). Two patients died soon after starting cytotoxic chemotherapy, and responses to the cytotoxic chemotherapy were assessed in 12 patients. In terms of the best response, eight patients (8/12, 67%) achieved an objective response during cytotoxic chemotherapy. Specifically, three patients achieved a complete response (CR) and five achieved a partial response (PR). Besides, remaining four patients (4/12, 33%) achieved a stable disease (SD) response as the best response to cytotoxic chemotherapy.
Among three patients achieving CR during the first course of chemotherapy, two survived for more than five years. Compared to the deceased patients, the two long-term survivors did not have lung metastasis, and their tumor burden was also much lower with fewer metastatic lesions. Furthermore, the two long-term survivors had their primary tumor surgically removed. Specifically, one patient had a brain tumor without a distant metastatic lesion and underwent surgical tumor removal and two courses of cytotoxic chemotherapy due to relapse after the first course of chemotherapy. The other patient had a testicular tumor with only some retroperitoneal lymph nodes involved and underwent radical orchiectomy and one course of cytotoxic chemotherapy.
On the other hand, one patient who died after achieving CR during the first course of chemotherapy had a testicular tumor with lung metastasis and hemoptysis. He died due to the progression of lung metastasis and subsequent respiratory failure despite receiving subsequent chemotherapy. Furthermore, all patients who achieved PR or SD to cytotoxic chemotherapy eventually died after developing resistance to chemotherapy.
We analyzed the association between clinical characteristics and OS (Table 3). The median OS was similar between the testicular and mediastinal PCC patients (13 months vs. 8 months, p=0.294). The median OS was lower in patients with hCG levels higher than 100,000 mIU/mL compared to those with hCG levels lower than 100,000 mIU/mL (5 months vs. 20 months, p=0.021). This means that patients with lower tumor burden are more likely to live longer because the level of hCG reflects the tumor burden of the choriocarcinoma. On the other hand, the median OS was similar between patients with increased AFP levels and those with normal AFP levels (12 months vs. 13 months, p=0.493).
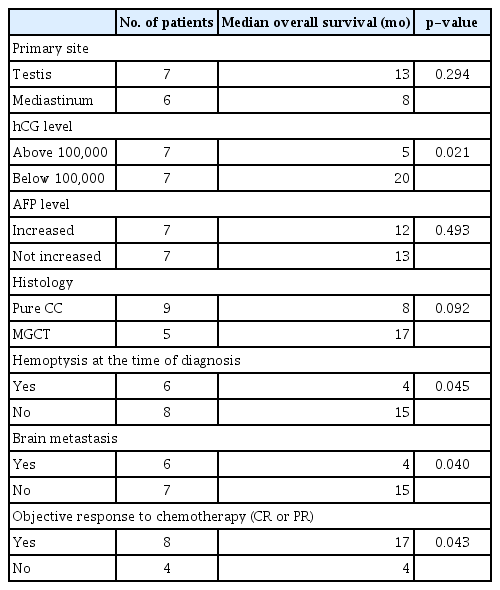
The association between clinical factors and overall survival in male patients with primary choriocarcinoma
The median OS was lower in patients with pure choriocarcinoma compared to those with MGCTs containing choriocarcinoma, but not statistically significant (8 months vs. 17 months, p=0.092). This result may be derived from the association between hemoptysis at the time of diagnosis and pure choriocarcinoma histology (p=0.031). Indeed, the median OS was lower in patients with hemoptysis at the time of diagnosis compared to those without hemoptysis (4 months vs. 15 months, p=0.045). Additionally, there was no hemoptysis in patients with MGCTs containing choriocarcinoma at the time of diagnosis. Except for one patient with a brain tumor without distant metastatic lesions, the median OS was lower in patients with brain metastasis than in those without brain metastasis (4 months vs. 15 months, p=0.040). In the case of lung metastasis, only one of the deceased patients was free of lung metastasis at the time of diagnosis, but lung metastasis occurred during treatment. These results suggest that survival is shorter in patients with metastasis to organs that are prone to cause clinically threatening symptoms, such as the lungs and brain.
Among patients whose response to chemotherapy could be evaluated, median OS was higher in patients who achieved an objective response to cytotoxic chemotherapy compared to those who did not (17 months vs. 4 months, p=0.043). Indeed, one patient with hemoptysis at the time of diagnosis survived for 20 months, probably due to achieving CR with cytotoxic chemotherapy.
Discussion
To date, there is no standard treatment for the management of male patients with PCC [7]. Cytotoxic chemotherapy is considered an essential treatment, although a variety of treatment strategies, such as surgery and radiotherapy, are also considered. In our study, all 14 patients received cytotoxic chemotherapy, of whom 12 patients with recorded responses achieved either objective response or SD as the best response to chemotherapy. However, 10 of the patients eventually died after developing resistance to chemotherapy. These results suggest that most male patients with PCC will become resistant to chemotherapy during therapy, leading to treatment failure.
Immune checkpoint inhibitors (ICIs) have been used in the treatment of many types of cancer [9]. ICIs typically include anti–cytotoxic T-lymphocyte antigen-4 antibodies, anti–programmed death-1 (PD-1) antibodies, and anti–programmed death-ligand 1 (PD-L1) antibodies. Among those, anti–PD-1 antibodies and anti–PD-L1 antibodies target the PD-1/PD-L1 pathway. Blocking the PD-1/PD-L1 inhibitory pathway is thought to activate T cells in the tumor microenvironment, releasing inflammatory cytokines and cytotoxic granules to eliminate tumor cells. Currently, the expression levels of PD-L1 in tumor tissues is considered as a biomarker for predicting the responsiveness to PD-1/PD-L1 blockade therapy.
Recently, Veras et al. [10] reported PD-L1 expression in human placentas and gestational trophoblastic diseases, including choriocarcinoma. In human placentas, syncytiotrophoblasts highly express PD-L1, whereas cytotrophoblasts do not, and intermediate trophoblasts express little or no PD-L1. The authors suggested that trophoblastic cells in the placenta contribute to the creation of a tolerogenic feto-maternal interface by upregulating PD-L1 in syncytiotrophoblasts and intermediate trophoblasts. The authors also reported that 22 of 30 choriocarcinoma specimens (73%) showed intense and diffuse PD-L1 immunoreactivity in syncytiotrophoblasts. The other samples showed weak or no PD-L1 staining, which was attributed to the fact that most of the tissues were necrotic, and only a few viable trophoblasts were present. The typical pattern of choriocarcinoma is known as a plexiform arrangement of syncytiotrophoblast cells with mononucleated, mostly cytotrophoblast cells around the foci of the hemorrhage, although some cases may have a relatively inconspicuous syncytiotrophoblast component [4]. These findings suggest that PD-L1 expression from syncytiotrophoblast cells in choriocarcinoma might contribute to immune tolerance against anti-tumor T cells.
Several studies have been conducted on the efficacy of PD-1/PD-L1 blockade therapy on trophoblastic neoplasia, including choriocarcinoma [11–13]. Ghorani et al. [11] reported four cases of drug-resistant gestational trophoblastic neoplasia treated with pembrolizumab. In this study, all four cases had PD-L1 overexpression, but three out of four patients achieved remission. It was thought that one patient did not respond to pembrolizumab due to the absence of tumor-infiltrating lymphocytes.
Moreover, there are some reports on the efficacy of PD-1/PD-L1 blockade therapy on male PCC. Chi et al. [14] reported that one male patient with PCC achieved a partial but durable response to nivolumab treatment. Loh and Fung [15] reported that one male patient with PCC did not respond to pembrolizumab treatment and progressed rapidly. In these two cases, both PD-L1 overexpression and the presence of tumor-infiltrating lymphocytes were not evaluated. Han et al. [16] reported that one male patient with PCC achieved remission after pembrolizumab treatment combined with cytotoxic chemotherapy. In this study, PD-L1 overexpression on tumor cells was confirmed. On the other hand, in a study by Adra et al. [17], only one of three male PCC patients showed PD-L1 overexpression, and none of the three patients achieved an objective response to pembrolizumab treatment. These results suggest that PD-1/PD-L1 blockade therapy is not effective in all male patients with PCC. It is thought that the therapeutic efficacy of PD-1/PD-L1 blockade varies depending on some clinicopathological features such as PD-L1 overexpression and the presence of tumor-infiltrating lymphocytes.
In summary, there is no established standard treatment for male PCC, and cytotoxic chemotherapy is used as a mainstay treatment. Although some patients with low tumor burden and only few metastases can be cured by cytotoxic chemotherapy, most male PCC patients will eventually develop resistance to cytotoxic chemotherapy and die from disease progression. Factors such as poor response to chemotherapy, high disease burden, brain metastasis, and hemoptysis at the time of diagnosis might all be poor prognostic factors associated with shorter survival time. ICIs, such as anti–PD-1 antibodies and anti–PD-L1 antibodies, can be a salvage treatment for chemotherapy-resistant male PCC patients. PD-L1 overexpression and the presence of tumor-infiltrating lymphocytes can be used as biomarkers for predicting the efficacy of PD-1/PD-L1 blockade therapy.
Notes
Ethical Statement
Study protocol was reviewed and approved by the Samsung Medical Center (Seoul, Korea) institutional review board (2020-05-072-001). Informed consent was waived by the institutional review board due to the retrospective study design.
Author Contributions
Conceived and designed the analysis: Ji YS, Park SH.
Collected the data: Ji YS, Park SH.
Contributed data or analysis tools: Ji YS, Park SH.
Performed the analysis: Ji YS, Park SH.
Wrote the paper: Ji YS, Park SH.
Conflicts of Interest
Conflict of interest relevant to this article was not reported.