Polymorphic Variants in Oxidative Stress Genes and Acute Toxicity in Breast Cancer Patients Receiving Radiotherapy
Article information
Abstract
Purpose
Reactive oxygen species (ROS) are generated as an indirect product of radiation therapy (RT). Genetic variation in genes related to ROS metabolism may influence the level of RT-induced adverse effects. We evaluated the potential association of single nucleotide polymorphism (SNP)–related response to radiotherapy injury in breast cancer patients undergoing RT.
Materials and Methods
Eighty patients receiving conventional RT were included. Acute effects were evaluated according to the Radiation Therapy Oncology Group (RTOG) scores. DNA was extracted from blood and buccal swab samples. SNPs were genotyped for GSTP1, GSTA1, SOD2, and NOS3 genes by polymerase chain reaction–based restriction fragment length polymorphism. Univariate analysis (odds ratios [ORs] and 95% confidence interval [CI]) and principal component analysis were used for correlation of SNPs and factors related to risk of developing ≥ grade 2 acute effects.
Results
Sixty-five patients (81.2%) showed side effects, 32 (40%) presented moderate to severe acute skin toxicity, and 33 (41.2%) manifested minimal acute skin reactions by the end of treatment. In both univariate and multivariate analyses, nominally significant associations were found among body mass index (OR, 3.14; 95% CI, 8.5338 to 1.1274; p=0.022), breast size (OR, 5.11; 95% CI, 17.04 to 1.54; p=0.004), and grade ≥ 2 acute radiation skin toxicity. A significant association was also observed between NOS3 G894T polymorphism (OR, 9.8; 95% CI, 211.6 to 0.45; p=0.041) and grade ≥ 2 acute radiation skin toxicity in patients with neo-adjuvant chemotherapy treatment.
Conclusion
The analysis of the factors involved in individual radiosensitivity contributed to the understanding of the mechanisms underlying this trait.
Introduction
Survival rates for breast cancer (BC) have improved significantly in recent years due to new treatment options. However, BC remains a major killer in industrialized countries [1]. In 2012, more than 408,000 women were diagnosed with BC in Latin America and 92,000 died from the disease. Current projections suggest a 46% increase during the next two decades. Therefore, early detection and treatment advances may improve management and survival of BC [2].
Radiation therapy (RT) is an important tool in the treatment of BC [3]. It has been accepted as a well-established protocol after breast conserving surgery (BCS) for local tumour control and to reduce the risk of loco-regional recurrence [4,5]. However, this procedure presents adverse reactions in normal tissue, which are commonly classified as early and late effects [6].
Acute effects occur during or shortly after treatment completion; they are usually reversible, manifest mainly in the skin and can range from mild erythema and desquamation to necrosis and ulceration. Late radiation toxicities can be permanent; they occur from 6 months to several years after treatment, and include subcutaneous fibrosis, athrophy, and vascular damage [5,7]. The observed reactions can be dose-limiting and may question a curative treatment intent. Considerable technical efforts have been made to improve the effective tumour dose and decrease the amount of normal tissue inevitably included in the treatment volume [8]. As a consequence, standard radiation doses may induce different levels of early and late side effects, and the normal tissue response of patients will vary substantially [5,8].
Interindividual variability in normal tissue radiosensitivity is a multifactorial trait. It depends on treatment parameters such as total radiation dose and schedule, on clinical factors such as age and lifestyle, and on a genetic component [9]. Normal tissue radiosensitivity is regarded as a complex polygenic trait resulting from the combined effects of multiple common single nucleotide polymorphisms (SNPs) with modest functional effects and low level of penetrance [10]. Several lines of evidence support a genetic basis for normal tissue radiosensitivity; however, the specific genetic determinants and the underlying molecular mechanisms are only partly understood [9]. The main candidate genes involved in the pathogenesis of radiotoxicity participate in mechanisms of DNA damage repair, pro-inflammatory response, oxidative stress, and damage sensing.
RT exerts its cytotoxic effects through direct ionization of DNA and the production of free radicals such as reactive oxygen species (ROS) formed by radiolysis of water. These ROS react with cellular macromolecules, especially DNA. Thus, genetic variants in genes involved in protection from oxidative stress could explain the increased acute toxicity, i.e., higher incidence of erythema after a single dose [8]. Overexpression or diminished activity of antioxidant enzymes may strengthen the effectiveness of RT [1].
The enzymes that play a key role are manganese superoxide dismutase (SOD2), whose presence in the mitochondria enables the dismutation of superoxide radicals to hydrogen peroxide and oxygen, glutathione S-transferases (GSTs alpha, mu, pi, and theta), which neutralize ROS, and prooxidant enzyme endothelial nitric oxide synthase (NOS3), involved in the generation of reactive nitrogen species [11]. Few studies have evaluated the relationships of polymorphisms in oxidative stress–related candidate genes and acute toxicity, while some independent studies have confirmed correlation between them [1]. Nevertheless, some reports support that SNPs in genes related to oxidative stress influence the occurrence of acute skin toxicity in patients with BC [9,12]. However, more research is needed to confirm the involvement of specific genetic variants.
In view of the above mentioned, we evaluated the association of SNPs in genes related to enzymes involved in antioxidative activities (GSTP1, SOD2, NOS3, and GSTA1) and the development of RT adverse acute effects in BC patients.
Materials and Methods
1. Subjects and data collection
The current prospective study was conducted with patients from La Plata city and surrounding areas attending the Oncology Integrated Center, La Plata, Argentina. Eighty samples were obtained from individuals with histologically confirmed BC and after BCS (mean age, 59 years; age range, 26 to 79 years). The surgical procedure was quadrantectomy in 83.75% of cases; 31.25% of patients had previously undergone chemotherapy with anthracyclines and taxanes or a combination of both. Peripheral blood (5 mL in 5% ethylenediaminetetraacetic acid tubes) and buccal swabs were collected. Clinical data (age, body mass index [BMI], breast size, history of diabetes, hypertension, smoking status, alcohol, and adjuvant treatments) were obtained at the time of patient recruitment.
Patients were administered whole breast RT with conventional fractions (50-50.4 Gy, 1.8-2 Gy/fraction) followed by a 12-18 Gy electron boost. In most cases, irradiation was performed with photon beams from a 4 MeV linear accelerator using 3-dimensional conformal RT (3D-CRT) and in 7.5% with 2-dimensional radiation therapy (2D-RT) for planning. All treatments were equivalent in terms of biologically effective dose.
The acute side effects of RT developing in the skin within the radiation field of the breast were used for measurement of clinical radiosensitivity. The severity of these reactions was assessed using the scoring system of the Radiation Therapy Oncology Group (RTOG) criteria. Development of acute side effects grade ≥ 2 was considered to indicate increased sensitivity for acute effects. Patients with minimal or no skin reactions (grade < 2) were included in the control group. Grade 2 was defined by at least one marked erythema or moist desquamation, grade 3 as confluent moist desquamation or severe edema, and grade 4 was defined by ulceration, hemorrhage, or necrosis. The occurrence and severity of acute skin reactions were determined during and after RT, given the highest degree of toxicity.
The research protocol was approved by the Ethics Committee of the Human Genetics Association and was conducted in agreement with the Helsinki Declaration. Informed consent was obtained from patients before inclusion in the study and sample collection.
2. DNA extraction and genotyping of polymorphisms
The SNPs selected and their dbSNP ID (rs) were as follows: GSTP1 Ile105Val (rs1695), SOD2 V16A (rs4880), NOS3 G894T (rs1799983), and GSTA1 C69T (rs3957356). Total genomic DNA was extracted from blood leukocytes and swabbing oral mucosa. DNA quality was evaluated by spectrophotometer analysis (Nanovue, GE Heathcare, Buckinghamshire, UK). Samples were centrifuged at 12,000 rpm for 4 minutes. The supernatant was discarded, followed by successive washes with TE buffer (10 mM Tris-HCl, 0.1 mM EDTA) for removal of all traces of erythrocytes. The cell pellet obtained from the samples was incubated for 24 hours at 56°C in 300 μL of extraction buffer (50 mM Tris-HCl pH 8.5, 1 mM EDTA, 1% Triton X-100, and 0.5% Tween 20) and 10 μL of proteinase K (10 mg/mL, Promega, Madison, WI). Proteinase K was |inactivated by boiling for 10 minutes. DNA samples were stored at –20°C until use; 3 μL DNA were then used in performance of polymerase chain reaction (PCR) amplifications.
Polymorphisms were determined using the PCR-based restriction-fragment-length-polymorphism technique. PCR was performed in a total reaction volume of 25 μL using Taq DNA polymerase (Genbiotech, Buenos Aires, Argentina). Primer pairs were used at a concentration of 0.5 pmol/μL (Table 1). For all polymorphisms, cycling conditions were 94°C for 3 minutes, followed by 35 cycles of 94°C for 30 seconds, 55-57°C for 30 seconds, and 72°C for 30 seconds, with a final extension of 72°C for 3 minutes. PCR-products harboring the SNPs were digested overnight with 5 U of restriction enzymes (total volume, 15 mL; New England Biolabs, Ipswich, MA; Thermo Fisher Scientific, Fremont, CA) at the recommended temperatures. Digestions were as follows: GSTP1 with Alw26I to yield fragments of 83 bp and 93 bp; NOS3 with MboI (87 bp and 119 bp), SOD2 with BsaWI (74 bp and 85 bp), and GSTA1 with MnII (77 bp and 70 bp). They were resolved on 8%-10% polyacrylamide gels and visualized after staining with ethidium bromide.

Features of polymorphism genotyping
3. Statistical analyses
Each polymorphism was tested for deviation from Hardy-Weinberg equilibrium (HWE) by comparing the observed and expected genotype frequencies using Pearson’s chi-square test. The effect of clinical factors and genetic variables on the risk of RT-induced acute skin toxicity was evaluated by univariate logistic regression analysis. Odds ratios (ORs) and their 95% confidence intervals (CI) were used as estimates of relative risk. Variables were analyzed by calculating correlations. Principal component analysis was used to determine the degree of association between variables and which variables contributed to variations in radiotoxicity. Statistical analyses were performed using the IBM SPSS ver. 19 (IBM Co., Armonk, NY).
Results
1. SNPs and radiotoxicity
Sixty-five patients (81.2%) presented adverse side effects, 32 (40%) experienced moderate to severe acute skin toxicity (RTOG grade 2-4), while 33 (41.2%) manifested minimal acute skin reactions (RTOG grade 1). Pulmonary toxicity was not recorded in any of the patients.
All genotype distributions were in HWE both in control and in individuals with radiodermitis grade ≥ 2 (p > 0.05).
The observed minor allele frequencies of GSTP1, NOS3, SOD2, and GSTA1 were compared with those reported for the American population from phase 1 of the 1000 Genomes Project in the dbSNP database (Fig. 1).
Distribution of each allele for studied genes. Obs, observed; Exp, expected; AMR, American.
The results of univariate analysis showed no significant association of the polymorphisms in oxidative stress genes with risk for development of acute skin reactions (cut-off p-value < 0.05) (Table 2) in the patients studied. On the other hand, in analysis of only patients treated with neo-adjuvant chemotherapy (n=25, 31.25%), homozygous carriers of the NOS3 894T allele (OR, 9.8; 95% CI, 211.6 to 0.45; p=0.041) were at higher risk of developing acute skin reactions. However, no statistically significant OR was observed with other SNPs in this group.
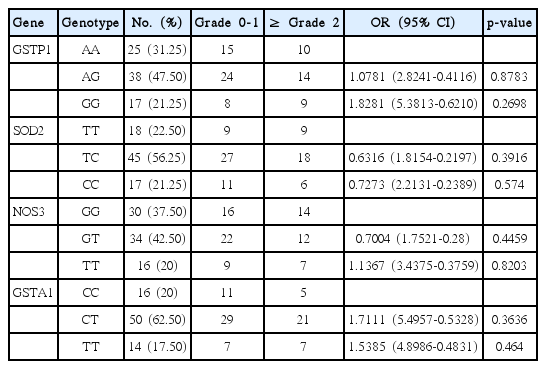
Association between GSTP1, SOD2, NOS3, and GSTA1 polymorphisms and risk of developing acute skin toxicity after RT in BC patients
2. Other factors affecting radiotoxicity
The clinical characteristics of patients are listed in Table 3. Mean age was 59.44 years. Older women presented higher radio-toxicity. Differences were observed in 33 patients grade ≥ 2 (mean age, 66.30 years) and 47 patients grade < 2 (mean age, 58.87 years).

Clinical and demographic characteristics of BC patients
None of the patients reported previous therapeutic exposure to ionizing or non-ionizing radiation, except for one who had undergone radiotherapy twice in the same breast with a 38-month interval between treatments who presented significant radiotoxicity (grade 4).
The reported vitamin and dietary supplements consumed by patients, individual factors including smoking habits, alcohol consumption, anemia, hypertension, diabetes, and severe acute radiotoxicity were not significant (data not shown). However, we found a positive correlation of BMI (OR, 3.14; 95% CI, 8.5338 to 1.1274; p=0.0222) and breast size (OR, 5.11; 95% CI, 17.04 to 1.54; p=0.004) with acute skin reactions. Thus, patients with BMI > 25 kg/m2 and medium and large breast were at greater risk of developing radiodermitis.
In addition, when comparing type of treatment (2D-RT and 3D-CRT) and radiotoxicity, no significant differences were observed (OR, 1.44; 95% CI, 8.37 to 0.25; p=0.68).
Discussion
This is the first study conducted in our country for analysis of gene variants related to DNA damage response pathways after ionization radiation on the risk of developing acute skin radiation toxicity in patients with BC receiving RT after BCS. These reactions can affect the therapeutic program and worsen the patient quality of life [4,12].
Individual radiosensitivity is a phenotype that can occur in several phases of treatment. Because its intensity depends on RT-related factors and individuals, we characterized different parameters in our population and correlated them with radio-induced skin reactions.
According to Schnur et al. [13], the majority of BC patients (74%-100%) will experience radiodermitis during the course of RT. Our results agree with the above mentioned results since 81.2% of our patients had skin toxicity, with a higher incidence of grades 1 and 2 (68.8%) compared with grades 3 and 4 (12.5%) (Table 3).
As indicated by radiation oncologists, grades 1 and 2 are usually tolerated by the patient, who can continue with RT. However, the toxicity of grades 3 and 4 requires the suspension of treatment and intervention with therapeutic agents. In this study, all patients concluded with the total dose planned. The pathogenesis of normal tissue is a dynamic process initiated in response to cell death. In recent years, the role of free radicals in the maintenance of chronic stress which interferes with the recovery of normal tissue has been evaluated. The emerging concept holds that there is no recovery of chronic tissue damage caused by ROS, pro-inflammatory cytokines and chemokines, which result in progressive damage and end in tissue injury [14]. Considering the pathways previously mentioned and that radiosensitivity is a polygenic trait, in this study the genes analyzed were selected based on their role in the establishment of antioxidant status. Thereby, we began evaluating SNPs GSTP1 Ile105Val (rs1695) and GSTA1 C69T (rs3957356). The low activity variant of GSTP1 was associated with a greater than 2-fold risk for acute reactions of the irradiated skin in BC patients [15]. In addition, Falvo et al. [16] reported a protective role as a trend for wt GSTP1. However, and the same as in another report [17], in this study no statistically significant association was observed between GSTP1 and radiosensitivity. On the other hand, an association between GSTA1 (rs3957356) and adverse skin effects could not be demonstrated. Opposite to this, Falvo et al. [16] reported an association between wt GSTA1 and erythema, and Ambrosone et al. [15] found this allele as a protective agent.
Regarding SOD2 gene, none of the genotypes was associated with risk of radiotoxicity, in coincidence with Ahn et al. [12]. However, Ambrosone et al. [18] found that genotypes related to higher oxidative stress were associated with better BC survival.
Finally, we found association between acute radiotoxicity and NOS3 homozygous T allele in patients who received neoadjuvant chemotherapy. The enzyme NOS3 catalyzes the production of the free radical nitric oxide (NO), and the 894G>T variant in the NOS3 gene results in a 298Glu>Asp substitution that alters susceptibility to cleavage and leads to reduced NO levels [19]. Probably, the decreased NO would produce a lower vasodilator mediated effect and, consequently, a lower intake of oxygen and nutrients needed for tissue reconstruction. Likewise, it could exacerbate chemotherapy-induced damage in situ, considering that anthracycline-mediated oxidative stress is responsible for membrane lipid peroxidation. This free radical activates the immune system, which is central to the establishment of RT side effects [14]. Because this trait is influenced by quantitative genetics, a multivariate analysis was performed, without achieving positive correlations. This is in line with most studies in BC patients [20] showing no significant association between the vast majority of SNPs and acute effects.
In addition to genetic analysis, others factors influencing the development of radiosensitivity were considered, including the clinical data recorded and the characteristics associated with treatment. In the case of the age of patients, older women presented higher toxicity. These results argue against other studies suggesting that RT is well tolerated in old patients [21]. Concerning smoking, no significant association was found, probably due to the low incidence of smokers in this population. In the case of hypertension, at least 38% of patients were hypertensive, and no statistical significance was observed with relation to the severity of skin reactions. Only 8% of patients presented with diabetes. However, no other study has shown diabetes as a predisposing factor for adverse skin reactions [21,22]. In agreement with these results, Terrazzino et al. [9] reported that no solid that diabetes mellitus, hypertension or smoking status were predisposing factors for acute radiosensitivity [22,23].
Among other clinical features investigated, the results of multivariate analysis showed that breast size and BMI were predictors of acute skin toxicity, in agreement with Terrazzino et al. [9]. Several studies consider that breast size is important because the volume irradiated is a factor related to radiation and interferes in the incidence and severity of side effects. Larger breast volumes require application of larger doses on the skin to reach the desired dosage in tissue and deeper structures [9,21]. Our results substantiate those showing a more intense skin reaction in medium and large breasts [24]. In addition, Twardella et al. [25] previously reported an association of overweight/obesity (BMI > 25 kg/m2) with an increased risk of acute radiotoxicity. In relation to this parameter, whereas individuals with normal BMI presented one third of acute effects grade ≥ 2, overweight/obesity patients showed half of these effects.
Conclusion
Given the importance of BC as a frequent pathology in our region, studies are important not only to improve prevention but also to optimize treatment. In relation to RT, it is important to elucidate the mechanisms underlying radiotoxicity as well as to establish or confirm associations between genetic variants and risk of developing severe acute effects. Our results could not prove the association between radiotoxicity and oxidative stress genes, due in part to the small sample size and the low penetrance alleles. However, considering that radiotoxicity is a multifactorial trait, the participation of other mutations in these genes or in sequences regulated by them, epigenetic changes or other candidate genes cannot be excluded.
Notes
Conflict of interest relevant to this article was not reported.
Acknowledgements
The authors gratefully acknowledge the study participants for their cooperation and voluntary participation. Thanks are also due to the team of doctors, medical physicists, and administrative staff of the Integrated Oncology Center for their assistance in this study. E.E. Córdoba is a fellow of the Consejo Nacional de Investigaciones Científicas y Técnicas, Argentina. We also thank A. Di Maggio for language editing.