Introduction
Overall lung cancer survival rates have improved over the past few decades with the advances made in diagnostic and therapeutic modalities [1]. The use of low-dose computed tomography (CT) imaging has proved effective for early detection of lung cancer and consequent mortality reduction [2]. Moreover, the improvements in both local and systemic therapies, such as radiation therapy (RT), targeted therapy, and immunotherapy, have contributed to improved outcomes in lung cancer patients [1,3].
RT, one of the main treatment options, has played a key role in all stages of therapy, including as a curative modality for medically inoperable early-stage lung cancer and as a palliative tool for advanced and metastatic stages. The effects of RT are mediated by energy deposition and the genetic damage it causes to the cells it passes through, resulting in reproductive cell death during cell division. As it damages both cancer cells and surrounding normal cells, RT impairs anatomic barrier and immune response, which may cause infectious complications [4,5].
Chronic pulmonary infections (CPIs), such as pulmonary tuberculosis (PTB), non-tuberculous mycobacterial pulmonary disease (NTM-PD), and chronic pulmonary aspergillosis (CPA), usually occur in patients with underlying lung diseases. The risk factors for CPI include fibronodular lesions on chest images, the presence of bronchiectasis or chronic obstructive pulmonary disease (COPD), and sequelae of PTB [6–8]. Though the causal relationship between the development of lung cancer and CPI is not clearly proven, patients with CPI frequently also have a history of lung cancer. In a meta-analysis, lung cancer was associated with a 6-fold increase in PTB development, which was the type of cancer most frequently associated with PTB among the solid cancers [9]. Another previous study reported a three-fold higher prevalence of lung cancer in patients with NTM-PD than those without NTM-PD [10]. The incidence of CPA continues to rise, and CPA is often regarded as a form of complication following surgery for lung cancer [11,12]. As its cumulative incidence showed an increasing tendency proportionately with the length of follow-up, more focus on CPA development during post-treatment follow-up might be required in patients with risk factors.
Despite the increased reports of CPI together with improved survival rates among lung cancer patients, there have not been enough data collected on CPI following thoracic RT (TRT). In this context, we intended to investigate the cumulative incidence of CPI and the related risk factors following TRT in lung cancer patients at the authors’ institute.
Materials and Methods
1. Study design and population
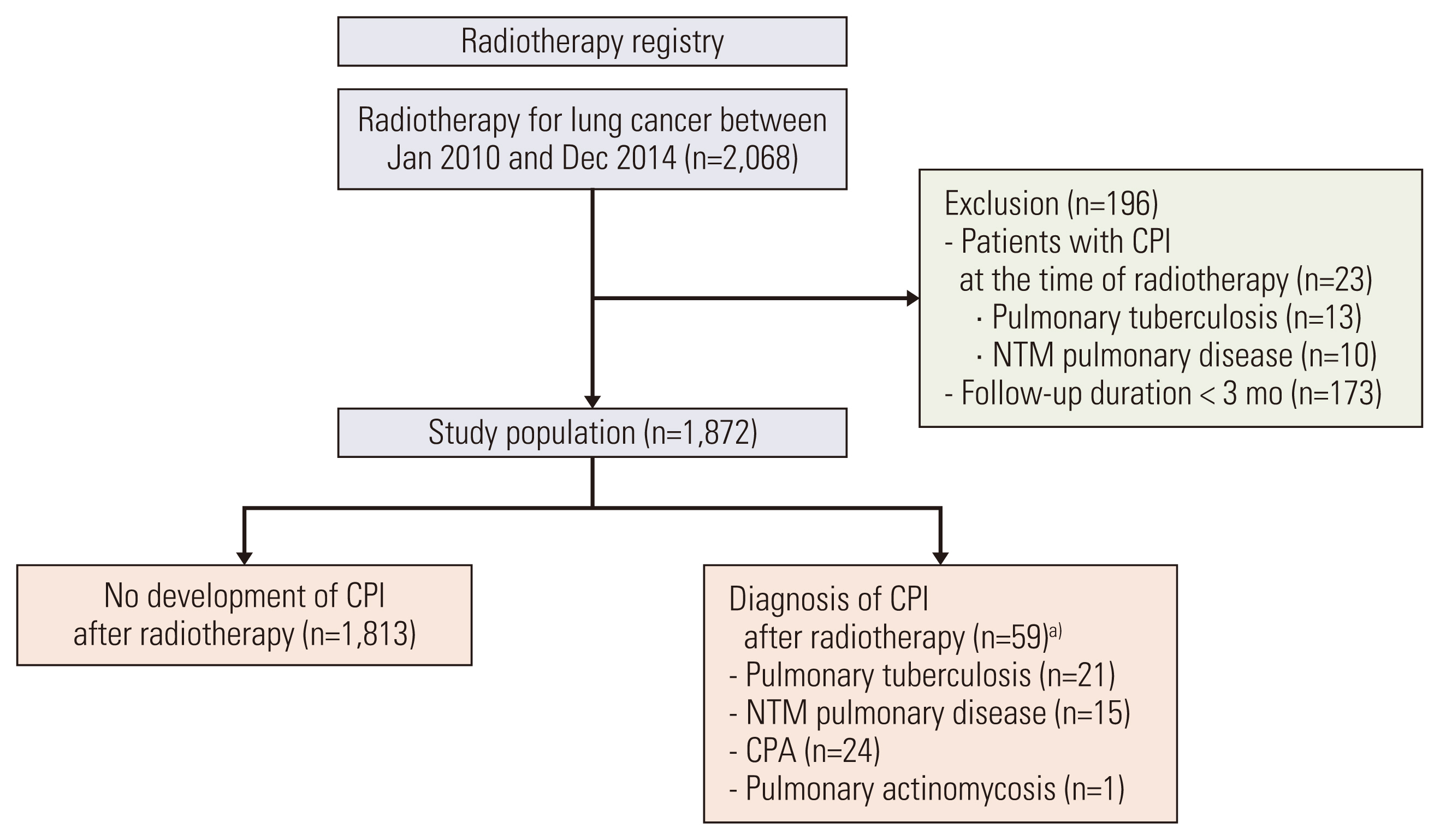
The records of 2,068 lung cancer patients who underwent TRT at Samsung Medical Center between 2010–2014 were retrospectively reviewed. After excluding 196 patients (23 who already had CPI at the time of TRT initiation and 183 who were followed up for < 3 months), 1,872 were enrolled in the current study (Fig. 1).
After RT for lung cancer, most patients were followed up by a radiation oncologist and chest CT scans were regularly performed during follow-up. Our institutional standard was to perform CT scans every 3 months for the first 2–3 years and then every 6 months up to 5 years unless recurrence was documented, and to obtain positron emission tomography computed tomography if needed. Patients with pre-existing or newly developed pulmonary disease and those with symptoms or signs of CPI were referred to a pulmonologist, and further diagnostic tests were performed. CPI was defined as PTB, NTM-PD, CPA, or pulmonary actinomycosis. The diagnosis of PTB was principally based on positive results of acid-fast bacilli (AFB) culture or polymerase chain reaction for Mycobacterium tuberculosis in respiratory specimens and included those cases in which clinicians decided to deliver a full course of anti-tuberculosis treatment [13]. NTM-PD was diagnosed by positive results of AFB culture from at least two separate sputum samples, positive results from at least one bronchial wash or lavage, or positive results from at least one respiratory specimen with mycobacterial histologic features following the guideline [14]. The diagnosis of CPA was based on compatible symptoms, direct or indirect microbiological evidence of Aspergillus species, and compatible radiological findings [15]. Pulmonary actinomycosis was diagnosed by the bacteriological identification of Actinomyces from a sterile respiratory specimen.
2. Data collection, clinical assessment, and outcomes
Patient characteristics, including age, sex, body mass index (BMI), smoking status, past medical history, comorbidities, prescribed medications, clinical stage and treatment history of lung cancer, and CPI development, were obtained from medical records. A systemic corticosteroid user was defined as a patient receiving more than 10 mg of corticosteroids daily or a cumulative dose of more than 700 mg of prednisolone or equivalent [16]. An inhaled corticosteroid (ICS) user was defined as a patient prescribed ICS for 30 days or longer. Clinically meaningful radiation pneumonitis was defined as grade 2 or higher pneumonitis in the current study according to the Common Terminology Criteria for Adverse Events, ver. 5.0, meaning symptomatic and requiring systemic corticosteroids. Clinical stages were assigned according to the eighth edition of the International Association for the Study of Lung Cancer proposal for tumor–node–metastasis classification for lung cancer.
3. Radiation therapy
The TRT techniques were selected individually based on the disease extent, the patients’ performance and cardiopulmonary functional status, and the estimated risk of pulmonary toxicity. For treatment planning, all patients underwent contrast-enhancing simulation CT scans in the supine position at a thickness of 2.5–5.0 mm. The Pinnacle3 system (ver. 8.0, Philips Medical Systems, Fitchburg, WI) was used to calculate the radiation dose. Patients were most commonly treated with three-dimensional conformal RT (3D-CRT; 85.5%), followed by intensity-modulated RT (8.7%) and stereotactic body RT (5.0%). The gross tumor volume (GTV) was defined as the volume of the tumor identified based on all available clinical information. The clinical target volume (CTV) was delineated by adding a 5-mm margin in all directions from the GTV, and the margins were modified in accordance with the adjacent organs when necessary. The 3D-CRT plan was usually composed of three or four photon beams of 4 to 10 MV to cover the CTVs plus 1.0 to 1.5 cm margins. A few different dose schedules were employed based on the clinical settings of TRT, whose comparative analyses were done by calculating biologically effective doses (BED10) using the following linear-quadratic formula with an α/β ratio of 10: BED10=nd×[1+d/(α/β)], where n equal to the number of daily fractions and d equals to the daily dose per fraction (Gy).
4. Statistical analysis
Data are presented as median with interquartile range (IQR) values for continuous variables and frequency and percentage values for categorical variables. Patients who developed CPI were compared to those without CPI using Pearson’s chi-squared test or Fisher’s exact test for categorical variables and the Mann-Whitney U test for continuous variables.
The cumulative incidence of CPI and overall survival (OS) were estimated using the Kaplan-Meier method. A multivariable Cox proportional hazards analysis with a backward stepwise selection with p < 0.05 for entry and p > 0.10 for removal was performed to identify risk factors associated with CPI development and calculate hazard ratios (HRs). The clinical stage of the tumor and indications of RT were not included in the multivariable analysis because they had significant collinearities with other variables for lung cancer treatment (concurrent chemoradiation and lung cancer surgery). Because most of the enrolled patients underwent 3D-CRT, the RT technique parameters could not be included in the multivariable analysis. In order to overcome the heterogeneity of the study population, we performed a subgroup analysis as follows: (1) excluding patients received salvage or palliative TRT (excluding patients with poor survival and low incidence of CPI); (2) patients received adjuvant or neoadjuvant TRT (almost all patients underwent surgery); and (3) patients received definitive TRT (almost all patients did not undergo surgery). All tests were two-sided, and p < 0.05 was considered statistically significant. SPSS ver. 25.0 (IBM Corp., Armonk, NY) was used for analysis.
Results
1. Cumulative incidence of CPI
With a median follow-up duration of 2.3 years (IQR, 0.9 to 5.0 years), the OS rates at 2 and 5 years following TRT were 55.6% and 37.6%, respectively (Fig. 2). During the follow-up period, CPI developed in 59 patients, including PTB in 21, NTM-PD in 15, CPA in 24, and pulmonary actinomycosis in one patient, respectively. The median time until CPI diagnosis was 1.8 years, and the cumulative incidence rates at 1, 3, 5, and 7 years were 1.1%, 3.4%, 5.0%, and 6.8%, respectively.
2. Baseline characteristics in relation with TRT
The median age of all patients was 63 years (IQR, 56 to 70 years), and there were higher numbers of male patients (78.3%), ever-smokers (78.2%), and patients with stage III non–small-cell lung cancer (50.5%), respectively (Table 1). Among all study participants, 903 patients (48.2%) had medical comorbidities, and those who developed CPI more frequently had previous PTB infections (13.6% vs. 1.7%, p < 0.001), chronic heart disease (33.9% vs. 19.3%, p=0.006), COPD or asthma (22.0% vs. 12.6%, p=0.033), and diabetes mellitus (30.5% vs. 19.5%, p=0.037), respectively.
Table 2 shows the treatment details for TRT. Among all indications for TRT, the most common ones were definitive (45.4%), followed by preoperative (22.6%). Interestingly, CPI development was more frequently observed in patients who underwent preoperative TRT (45.8% vs. 21.8%) and had a history of surgery (61.0% vs. 44.8%, p=0.014), respectively. However, there were no differences in RT regimens between the two groups. The median prescribed total dose was 52.5 Gy (IQR, 44.0 to 60.0 Gy), the median BED10 was 63.5 Gy (IQR, 52.8 to 79.2 Gy), and the median CTV was 167 cm3 (IQR, 88 to 281 cm3). Reirradiation was performed in 270 patients (14.4%), and concurrent chemoradiation therapy was prescribed in 1,252 patients (66.9%). Radiation pneumonitis was more common in patients with CPI than those without CPI (27.1% vs. 13.1%, p=0.002). Although there was no statistically significant difference in the proportion of systemic corticosteroid users (78.0% vs. 70.3%, p=0.202), ICS use was more common among patients with CPI than those without CPI (35.6% vs. 11.6%, p < 0.001).
3. Risk factors of CPI
Factors related to CPI development were identified using univariable and multivariable Cox proportional hazards analyses (Table 3). A previous PTB infection (HR, 5.81; 95% confidence interval [CI], 2.61 to 12.94; p < 0.001), ICS usage (HR, 3.31; 95% CI, 1.90 to 5.77; p < 0.001), a history of radiation pneumonitis (HR, 2.87; 95% CI, 1.55 to 5.32; p=0.001), interstitial lung disease (HR, 3.53; 95% CI, 1.34 to 9.28; p=0.010), lower BMI (per 1-kg/m2 increment; HR, 0.89; 95% CI, 0.82 to 0.98; p=0.015), a history of lung cancer surgery (HR, 1.80; 95% CI, 1.02 to 3.17; p=0.042), and a larger CTV (per 10-cm3 increment; HR, 1.02; 95% CI, 1.00 to 1.03; p=0.047) were independently associated with the development of CPI. Fig. 3 shows cumulative incidence rates of CPI for these independent risk factors. Continuous variables such as BMI and CTV were presented after conversion to binary variables.
After excluding patients who received salvage or palliative TRT, the results of multivariable analysis were similar to those of the population (S1 Table). A previous PTB infection, interstitial lung disease, ICS usage, and a larger CTV were independently associated with the development of CPI in the subgroup who received neoadjuvant or adjuvant TRT (S2 Table), whereas a previous PTB infection, a history of radiation pneumonitis, and ICS usage were identified as risk factors in the subgroup who received definitive TRT (S3 Table).
Discussion
The associations of CPI with lung cancer have been well-recognized in previous studies. Fan et al [17]. reported that more than 25% of lung cancer patients had latent tuberculosis infections at the time of diagnosis, which can evolve into active PTB in 5%-10% of patients [9]. The prevalence of PTB was also reported as 1%-2% in surgically treated lung cancer patients [18]. More than 5% of NTM-PD patients also have a history of lung cancer, and these individuals tend to have an increased mortality risk [19,20]. In our previous report, the cumulative incidence of CPA was 3.5% at 10 years after lung cancer surgery [12]. Although the incidence of CPI after TRT is not well known, the statistic of 6.8% at 7 years recorded in this study can be considered a high enough value to support an increase in attention paid while observing patients’ progress after TRT.
Similar to previous studies, several characteristics were identified as risk factors for the development of CPI in this study. Patients with PTB, NTM-PD, or CPA have lower BMI more frequently than healthy controls, and a lower BMI itself is also related to the increased mortality in this population [21–23]. The inter-relationship between low BMI and CPI is well established, though the cause-effect relationship and exact time sequence is not clearly documented, and the same was observed in the patients who underwent TRT in our study. In addition, structural lung diseases, such as underlying interstitial lung disease and prior PTB infection, are also well-known risk factors for CPI development. Nachiappan et al. [7] reported that fibronodular lesions on chest image are an underlying lung condition related to the reactivation of PTB, and several studies have also suggested that a history of PTB is a risk factor for both NTM-PD and CPA [8,24]. Besides, conditions such as interstitial lung disease or structural change after lung cancer surgery were reported to be associated with CPI [12]. These findings seem comparable to those of our study, which also demonstrated a previous PTB infection, underlying interstitial lung disease, and a history of lung cancer surgery as independent risk factors for CPI development.
One of the important findings of this study is that RT-related factors contributed to CPI development. Previous studies have generally suggested that the target volume (or tumor volume) of RT is a clinically significant factor for recurrence or mortality. One study reported that a log base 10 of tumor volume is a predictive factor of locoregional failure in patients with locally advanced disease [25]. Another found that a pre-treatment GTV greater than 50 cm3, irrespective of target volume reduction after RT, indicated poor survival in stage III non–small-cell lung cancer [26]. The present study revealed that a larger CTV was correlated with an increased CPI risk (per 10-cm3 increment: adjusted HR, 1.02; p=0.047; ≥ 100 cm3: adjusted HR, 2.05; p=0.029). In addition, we found that radiation pneumonitis was associated with CPI development. This is one of the major toxicities of thoracic RT and occurs in 24%-47% of patients who received traditional RT [5]. The effect of RT is based on radiation-induced free radicals and oxidative stress resulting in tissue injury. Radiation pneumonitis develops when radiated tissue fails to recover from this injury and shows progressive and exaggerated responses after RT. Considering its pathogenesis and our findings, CPI development may be associated with failure in recovery process of irradiated tissue. Besides, RT can induce immunosuppression, which may contribute to CPI development. RT-induced damage is related to innate and adaptive immune response, such as activating dendritic cells and T cells, which facilitates antitumor effect. It can also promote immunosuppression by polarization of immunogenic macrophages to an immunosuppressive phenotype and inducing lymphocyte apoptosis [4]. In terms of the phases of RT-induced lung injury, lymphocytes show a pro-inflammatory phenotype in the acute phase within days to weeks, although the chronic phase is characterized by an anti-inflammatory response occurred in months to years after RT [27]. Given that the median time to CPI diagnosis in this study was 1.8 years, anti-inflammatory response in the chronic phase may contribute to the development of CPI.
The use of ICS has been the main treatment for asthma and COPD, which may increase the risk of pneumonia [28]. In our study, ICS use correlated with a high risk for CPI development. This observation is consistent with those of previous studies reporting that ICS users are at an increased risk of PTB and NTM-PD [29,30]. We also investigated whether the use of systemic corticosteroids is associated with CPI development. Although the association between the use of systemic corticosteroids and an increased incidence of CPI is relatively well-known [16], we found no significant relationship between the use of systemic corticosteroids and CPI development in our study. In our study, 70% of patients used systemic corticosteroids, mostly as a pre-medication for chemotherapy or treatment for radiation pneumonitis. Therefore, we assumed steroid use to be a confounding factor rather than an independent risk factor.
Because of the significant heterogeneity of the population, we performed subgroup analysis. However, the number of CPI cases included in each subgroup was too small, limiting the identification of independent risk factors. Nevertheless, a previous history of PTB infection and ICS usage were consistently identified as risk factors for CPI in the subgroup analyses. Whereas a history of radiation pneumonitis was a risk factor in patients receiving definitive TRT but not in patients receiving neoadjuvant or adjuvant TRT. It may be assumed that this difference is due to surgical resection of the source of CPI even if radiation pneumonitis occurs in patients receiving neoadjuvant TRT.
This study has a few limitations that could prevent generalization of our observations: it is retrospective in nature, based on a single tertiary referral hospital cohort, has potential selection bias, and reported a relatively small number of CPI events observed, respectively. As the investigative studies were mainly performed on those patients who developed suspicious symptoms or radiologic clues, the actual incidence rate of CPI following RT may have been underestimated. Moreover, there was insufficient information on patients’ performance status, comprehensive radiological and microbiological data, and detailed grades of RT pneumonitis that could be considered related to the development of CPI. Further prospective studies will be needed to investigate the relationship between CPI development and these variables.
In brief, through the current study, with a median follow-up duration of 2.3 years, the cumulative incidence of CPI at 7 years has been estimated as 6.8% in lung cancer patients who underwent TRT. Several risk factors for CPI development were identified in the current study, as follows: lower BMI, underlying interstitial lung disease, prior PTB, larger CTV, a history of lung cancer surgery or radiation pneumonitis, and ICS use, respectively. These, coupled with the recent trend of improved OS in lung cancer patients in Korea, signify the clinical relevance and importance of CPI as a form of late complication following TRT, which deserves close monitoring following TRT. Further prospective studies, however, with a larger number of patients and longer-term follow-up, may be warranted.
In conclusion, the cumulative incidence of CPI was about 7% at 7 years after RT for lung cancer and showed an increasing trend during the follow-up period. We identified the risk factors associated with the treatment of lung cancer (larger CTV and history of lung cancer surgery or radiation pneumonitis) as well as commonly known risk factors (lower BMI, underlying interstitial lung disease, prior PTB, and ICS use). Therefore, it is necessary to closely follow the development of CPI in lung cancer patients with risk factors after RT.