Introduction
The landscape of cancer treatment is changing rapidly due to remarkable advances in basic science and translational research, as well as clinical research and trials. Nonetheless, more patients with cancers are getting interested in complementary and alternative medicine (CAM) treatment options other than conventional medicine [1]. An example that the self-administration of veterinary anthelmintics called fenbendazole cured chemotherapy-resistant cancer was widely covered by the South Korean media in 2019 [2]. This event has agitated and perplexed terminal cancer patients, causing drug shortages in some areas.
Previous studies have delved into the incidence of CAM use, healthcare professionals’ attitudes toward CAM, and communication patterns that differ by nationality and cancer type [3–8]. In Korea, up to 85% of patients with cancer use one or more types of CAM [9]. Several studies examined the attitude of patients and their families toward CAM, types of CAM, costs of using CAM, sources of information, and how they discuss it with physicians [10] or compare it with Korean traditional medicine [11]. According to these studies, a wide gap exists between patients’ expectations regarding the efficacy of CAM, including improved chances of survival, and physicians’ concern about its side effects and negative consequences. This gap prevents physicians and patients from establishing trust and interacting through sincere and clear communication and impairs effective anti-cancer management [12,13]. Therefore, identifying the current status of CAM usage and its associated factors is critical to developing CAM usage guidelines [11]. Unfortunately, to our knowledge, very few researchers have devoted attention to this area of inquiry.
Online cancer support group (OCSG) participants are composed of heterogeneous members who are generally younger and have higher levels of education compared to face-to-face support groups [14–16]. Moreover, OCSGs provide several advantages to promote communication between cancer patients, as its members share different communication subjects and goals [16]. This is particularly true in South Korea, where there is increased diversity in OCSG member composition with internet penetration in over 95% [17], which can swiftly disseminate the anti-cancer anthelmintic issue through internet-based media.
Thus, this research found it reasonable to perform an online survey to gather basic information on the current level and features of CAM usage and the factors related to the use of anthelmintics in OCSG members. The survey results can provide physicians with effective tools to improve trust and strengthen meaningful interactions with cancer patients regarding CAM usage.
Materials and Methods
1. Study population
OCSG members diagnosed with cancer were invited to participate in the online survey via a notice on their OCSG boards or social network services. Patients older than 20 years, who can read and understand Korean language on their own, took part in the survey. However, those who left the survey incomplete or had duplicate access to the same Internet Protocol address were excluded from the analyses.
2. Questionnaire and measurement
The National Center for Complementary and Integrative Health divides CAM into five broad categories: alternative medical systems, mind-body therapies, biologically based practices, manipulative and body-based methods, and energy therapies [18]. The survey questionnaire was based on a 25-item questionnaire on CAM conducted in a previous trial [10] and was modified by adding questions on anthelmintics. It comprised single- or multiple-choice questions and open-ended answers in five parts as followings: (1) patient characteristics; (2) attitudes toward and experience with CAM; (3) source of information and reliability; (4) experience with anthelmintics; and (5) online health information literacy [19] and usage. The online survey was performed using the SurveyMonkey platform. To evaluate attitudes toward each item, we adopted a five-point Likert scale, ranging from strongly disagree (score 0) to strongly agree (score 4).
3. Statistical analysis
The sample size was calculated using a survey sample size calculator. According to the Korean Statistical Information Service, the prevalence of cancer was 845,373 in 2018 [20]. Therefore 221 patients were required with a 90% confidence level, a 6% sampling error, and a dropout rate of 15%.
Descriptive analyses were performed to determine baseline patient characteristics. Categorical variables were shown using frequencies and percentages, and comparisons were made using Pearson’s chi-squared test or Fisher’s exact test, as appropriate. Continuous variables were summarized as median values and interquartile ranges (IQR), and their comparisons were conducted using the Mann-Whitney U test. We used a multiple logistic regression analysis model to identify factors associated with anthelminthic usage. Variables from the univariate analysis with a p-value of < 0.05, age, and sex were entered into the model. All statistical analyses were performed using PASS/SPSS ver. 26 (IBM Corp., Armonk, NY). A two-sided significance level of 0.05 indicated statistical significance.
Results
1. Baseline characteristics
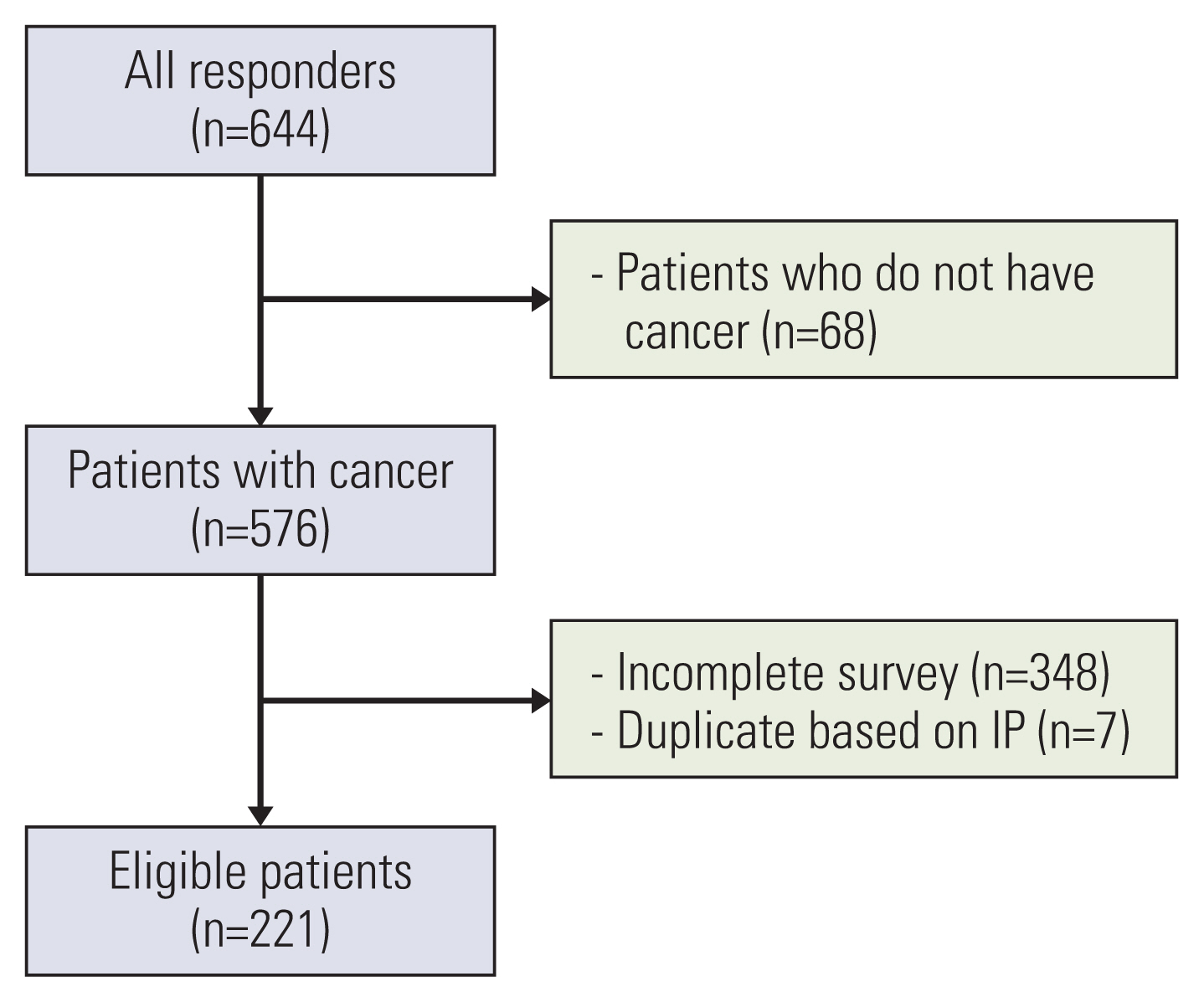
A total of 644 patients participated in the survey between August 18 and September 12, 2021; 34% (221 patients) completed the survey and were included in the analysis (Fig. 1).
Of the 221 eligible questionnaires, the median time taken for the survey was 17 minutes (IQR, 12 to 26 minutes). The median age of the patients was 52 years (range, 45 to 61 years), and 51.6% (114/221) of the total sample population were men. Of the patients, 99 (44.8%) lived in Seoul or metropolitan areas, and 95.9% were covered under the national health insurance. Of the total, 103 patients showed an Eastern Cooperative Oncology Group performance status of 0 (i.e., fully active without any restriction in performance). A total of 78.2% (173/221) of the patients had used CAM (Table 1), and 85.0% (147/173) initiated CAM after a cancer diagnosis.
Of the 155 CAM users who responded to the multiple-choice questions, 136 (87.7%) experienced biologically based therapies, followed by manipulative and body-based methods (50.3%), energy therapies (32.9%), alternative medical systems (25.8%), and mind-body therapies (18.1%). Of the 58 current users, 93.1% were under biological therapies, followed by energy therapies, manipulative and body-based methods, alternative medical systems, and mind-body therapies (Table 2).
2. Expectations and experiences regarding CAM use
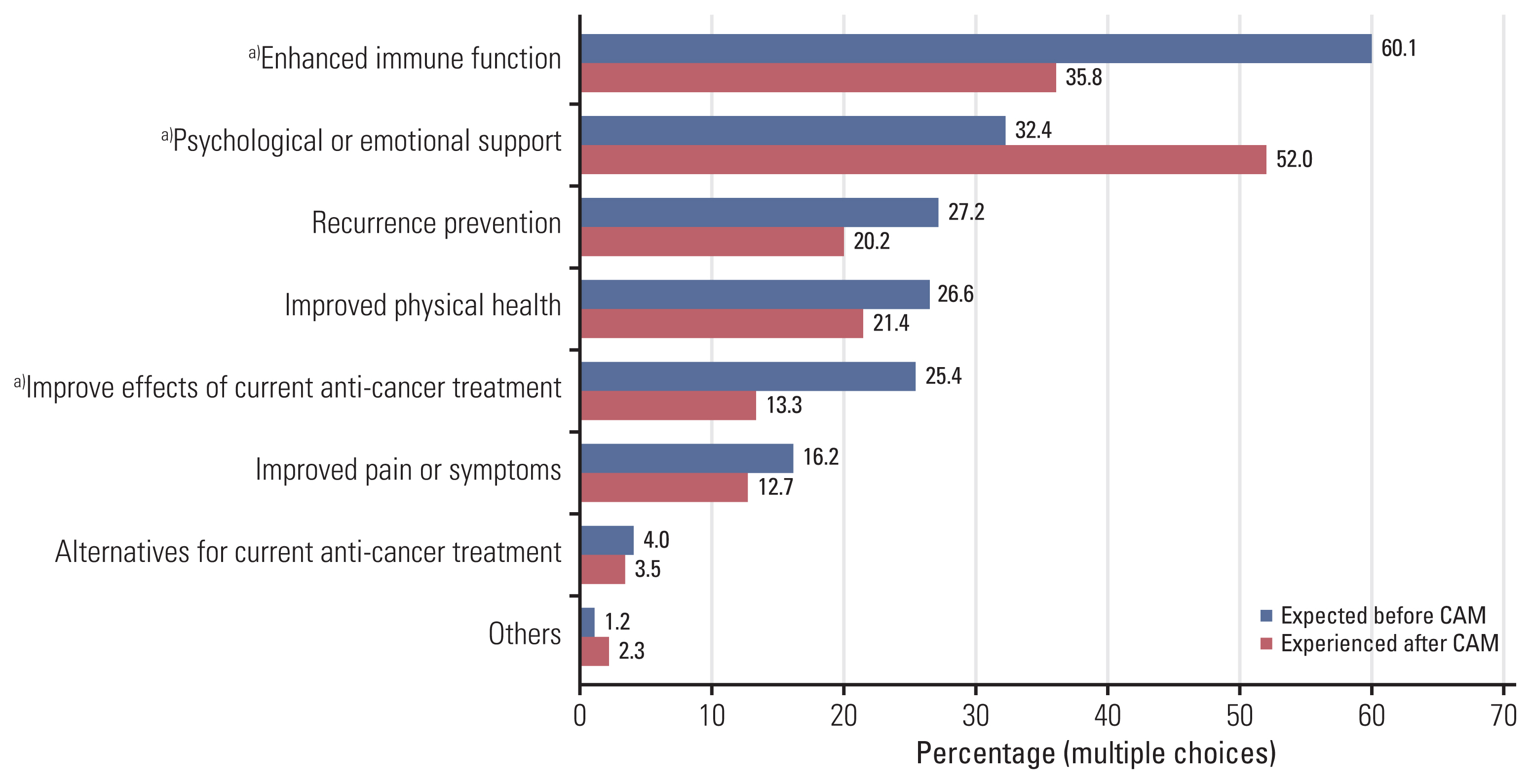
Based on their responses to the multiple-choice questions, a majority of the patients (60.1%) anticipated having an enhanced immune function, followed by psychological or emotional support (32.4%), recurrence prevention (27.2%), and improved physical health (26.6%). However, their feelings were considerably different from their expectations. They responded that psychological or emotional support was the most beneficial (52.0%), followed by enhanced immune function (35.8%), improved physical health (21.4%), and recurrence prevention (20.2%). Notably, they received much more psychological and emotional support from CAM use than was anticipated (32.4 vs. 52.0%, p < 0.001) (Fig. 2).
3. Source of information and reliabilities
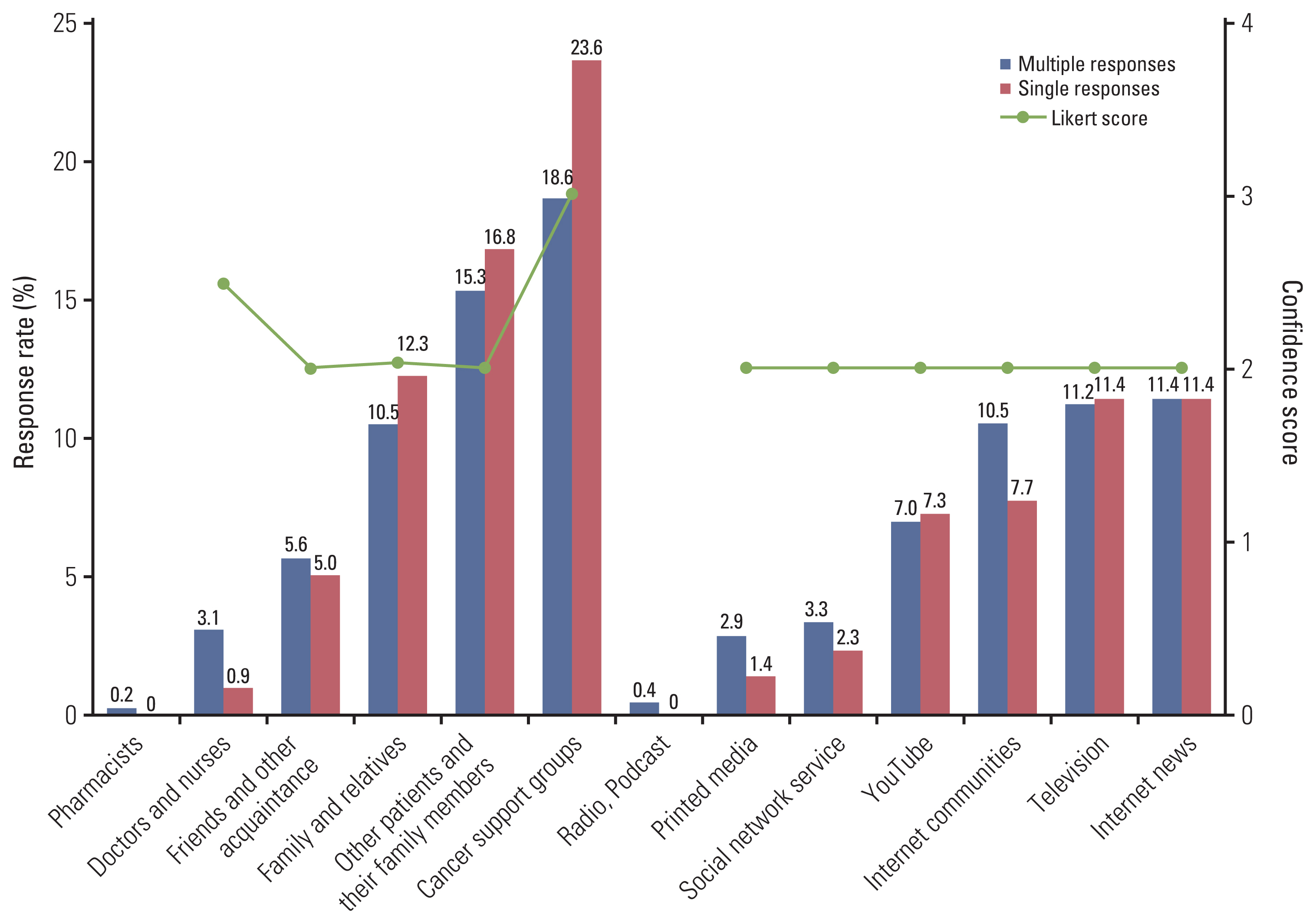
Two questionnaires were used for source of information and their reliabilities: one to indicate the most influential source (single) and the other to indicate every source encountered (multiple). The most common source of information was cancer support groups (single, 23.6%; multiple, 18.6%), followed by other patients or their family members (single, 16.8%; multiple, 15.3%), family or relatives (single, 12.3%; multiple, 10.5%), and Internet news (single, 11.4%; multiple, 11.4%). Interestingly, doctors and nurses had little impact on providing information (single, 0.9%; multiple, 3.1%). Furthermore, reliability measured by the Likert score was the highest in the online or face-to-face cancer support group (median, 3.0; IQR, 2.0 to 3.0), followed by doctors or nurses (median, 2.5; IQR, 2.0 to 3.0) (Fig. 3).
4. Discussion with physicians about CAM usage
Only 24.4% (54/221) of the patients discussed CAM with their physicians. Of the 173 patients who used CAM, 30.6% (53/173) discussed it with their physicians. When we asked the remaining 120 patients why they had not, 45 (37.5%) answered that their physicians would dislike the use of CAM, 22 (18.3%) assumed their physicians would prohibit its usage, and 16 (13.8%) thought it was not a matter to be discussed with their physicians (Fig. 4).
5. Use of anthelmintics and associated factors
Anthelmintics were used by 28 (16.2%) of the 173 CAM users. Younger age (odds ratio [OR], 0.89; 95% confidence interval [CI], 0.84 to 0.95), presence of metastasis (OR, 10.88; 95% CI, 3.39 to 34.86), previous exposure to CAM information (OR, 5.57; 95% CI, 1.01 to 30.72), number of CAM types used (OR, 1.98; 95% CI, 1.29 to 3.05), and CAM side effects (OR, 5.10; 95% CI, 1.46 to 17.75) were independently associated with increased use of anthelmintics, according to our multivariable analysis (Table 3).
Considering its spreading pattern, we approached anthelmintics usage from the aspect of online health information literacy. Based on the eHEALS [19], anthelmintic usage was not affected by online health information literacy (user vs. non-user, 30.1±4.6 vs. 28.6±4.5 [mean±standard deviation]; p=0.181).
6. Online health information use and efficacy among CAM users
Among the 173 CAM users, 26 patients (15.0%) started it before the cancer diagnosis, and 147 (85.0%) started it after the diagnosis. In light of online health information use, those who started it after the cancer diagnosis tended to think that they were well aware of the online health information and were more confident in finding useful online health information than those who started CAM before the cancer diagnosis (S1 Table).
Discussion
In this study, 78.3% of patients from the OCSG reported using CAM, and 16.2% of the CAM users utilized anthelmintics. Younger age, presence of metastasis, previous exposure to CAM information, number of CAM types, and the side effects experienced were independently associated with anthelmintic utilization. Users primarily obtained information online or from face-to-face cancer support groups, which showed the highest level of reliability. However, less than one-third of the patients discussed with physicians on CAM use.
In the previous study, 37.5% of patients with cancer were reported to use CAM [10]. Moreover, the Korean Health Panel data, which included the non-cancer population, revealed that 25.5% of patients with cancers used CAM [21]. However, the prevalence in our study was much higher (78.3%), and 85.0% of them started using CAM after the diagnosis. The high prevalence may be due to the peer influence of OCSGs inferred by cancer support groups’ highest accessibility and reliability. In addition, as survey participation was promoted through the internet and social network services, those with greater interest or experience with CAM were more likely to join. Moreover, the vulnerabilities and uncertainties they face as patients with cancers may partly explain it [4,21]. There is also a strong possibility that the anonymity of the survey would have resulted in candid answers.
Our finding that patients experienced more psychological and emotional support than expected is consistent with previous studies [22–24]. That is a positive side patient can feel. However, other answers, such as enhanced immune function, recurrence prevention, and improved physical health, cannot be objectively evaluated. Assumably, patients might have answered based on their feelings about the disease status at the time of the survey. Moreover, it is difficult to distinguish from the placebo effect and hard to find evidence that CAM affects health status. Conversely, it is hard to recommend CAM considering its side effects or financial toxicity [12,25].
This study’s finding that cancer patients obtain information mainly from non-healthcare professionals is also consistent with previous findings [10]. As cancer support groups and other patients and family members wield the most influence on decisions to use CAM, we should investigate their awareness, attitudes toward CAM, and relationship with patients. Although only a small proportion of patients gained information from doctors and nurses, they had higher credibility. Thus, communication between patients and medical professionals must be strengthened. Plans can be set up to guide patients in the appropriate direction for better care. Nevertheless, we found from another in-depth interview of patients that some physicians recommended CAM rather than conventional medicine, and more studies are needed to clarify the status (published elsewhere).
Among the studies with patients in western countries, the rate of discussion with physicians was 71.8% in the highest [26], but the revealing rate of most studies was low, up to 20% [10,23,27]. In our study, only 30% (53/173) of CAM users discussed it with physicians. Most attending physicians may not recognize their patients’ overall CAM usage status. Patients seemed not to disclose CAM usage owing to the fear of unfavorable reactions from physicians or that they might lack CAM knowledge or discourage the use. These reasons differ from those identified in a study conducted in the United States, where more than half answered, ‘The physician did not ask’ [10]. To ensure ethical considerations [28], phsicians should try to learn about CAM and more actively engage with their patients by asking questions and building rapport. Patients will then be encouraged to be sincere about actual remedies, which can protect them from unnecessary harm.
Recently, issues with anthelmintics usage among patients with cancer have been rampant, fueled by consumers influencing social media. Despite their lack of scientific background in specific drugs, they showed influential power in patients with terminal cancers. Even though experts and government organizations advised against using these drugs for cancer treatment, many patients were persuaded and took them as part of their treatment. Although the information on anthelmintics was widespread on the internet, we found that the actual use is unlikely to be influenced by online health information literacy. Conversely, younger age, presence of metastasis, previous exposure to CAM information, number of CAM types experienced, and side effect experiences were independently associated with anthelmintic use.
It is unclear why those who experienced side effects were more likely to use anthelmintics. However, we could assume that patients who experienced side effects from other types of CAM found alternatives for psychological or emotional support, even if it was under active debate. Therefore, physicians should regularly assess patients’ interest in CAM, provide accurate information, and manage them before they become more vulnerable as the disease progresses. Furthermore, they need to consider adopting protocols to disclose CAM usage [29].
Despite all these findings, our research has some limitations. First, there could be a selection bias due to the voluntary nature of the study and the limited spectrum of patients with cancer; not all OCSGs were willing to participate in the survey, and infrequent Internet users were less likely to be included, resulting in a lack of representativeness. Second, because of the nature of the survey, response bias may have been exacerbated in the online setting. It is possible that a more anonymous environment, as opposed to surveys with interviewers or paper surveys, would make patients feel free from societal norms, eliciting more honest answers. Third, despite our best effort to be neutral and structured, the order of the questionnaire may have resulted in question order bias, influencing the responses.
Even though information seemed to disseminate through the internet, younger age, presence of metastasis, exposure to CAM information, experience in more types of CAM, or side effects from CAM were associated with the use of anthelmintics rather than online health information literacy. Hopefully, our study will provide fundamental information for developing a CAM management strategy in this digital age.