Introduction
The health of the axillary lymph nodes comprises the singular most important prognostic factor within breast cancer, and the factor has widely been used in order to guide local-regional and systemic treatment decisions and the surgical removal of the axillary nodes facilitates staging, and additionally provides regional control within patients exhibiting axillary metastases. In recent years, sentinel lymph node (SLN) surgery has taken the place of axillary lymph node dissection (ALND) as the most widespread initial approach for treatment of women with clinically node-negative (cN0) disease, based upon the randomized trials demonstrating that SLN surgery is technically feasible in women exhibiting cN0 disease, which creates lower levels of morbidities like paresthesia, lymphedema, and the decreased range of motion associated with ALND [1,2].
Order to identify tumor metastasis within SLN, intraoperative techniques like frozen sections and imprint cytology are typically utilized; however, their sensitivities are generally less than optimal (63% and 78% for imprint cytology and frozen sections, respectively), and would worsen in the case of micrometastasis [3,4] and within patients administered neoadjuvant chemotherapy (NAC). As the false-negative rate of conventional intraoperative technique for sentinel lymph node dissection was demonstrated to be non-negligible [5], new, innovative diagnostic techniques are strongly recommended in order to minimize false negativity.
Various molecular diagnostic methods like reverse transcription polymerase chain reaction (RT-PCR) have previously been developed and examined for purposes of detecting tumor involvement. However, these specific techniques necessitate sophisticated and expensive instrumentation alongside specialized personnel, limiting the scope of their effectiveness and availability. Posed as a novel diagnostic tool, one-step nucleic acid amplification (OSNA) utilizing cytokeratin 19 (CK19) mRNA was employed and demonstrated to be suitable for purposes of the intraoperative evaluation of SLNs possessing a very low false-positive rate, a higher accuracy diagnosis of SLN status may be possible when it is combined with conventional histopathologic techniques.
Loop-mediated isothermal amplification (LAMP) comprises a novel nucleic acid amplification method that has widely been applied for purposes of the detection of various pathogen, but possesses the limitation of false-positive reactions via carry-over contamination due to its high sensitivity and productivity [6]. Still, the RT-LAMP method facilitates improved performance as compared to the intraoperative histology SLN evaluation, furthermore, direct reverse transcription loop-mediated isothermal amplification (direct RT-LAMP) method lacking RNA extraction is capable of being more efficient and comprises an easily accessible process.
In the present study, our team assessed the performance and efficacy of a direct RT-LAMP assay for purposes of the visual detection of CK19, CK20, and carcinoembryonic antigen (CEA) mRNAs in order to identify lymph node metastasis within patients exhibiting the early stages of breast cancer.
Materials and Methods
1. Patients and specimen
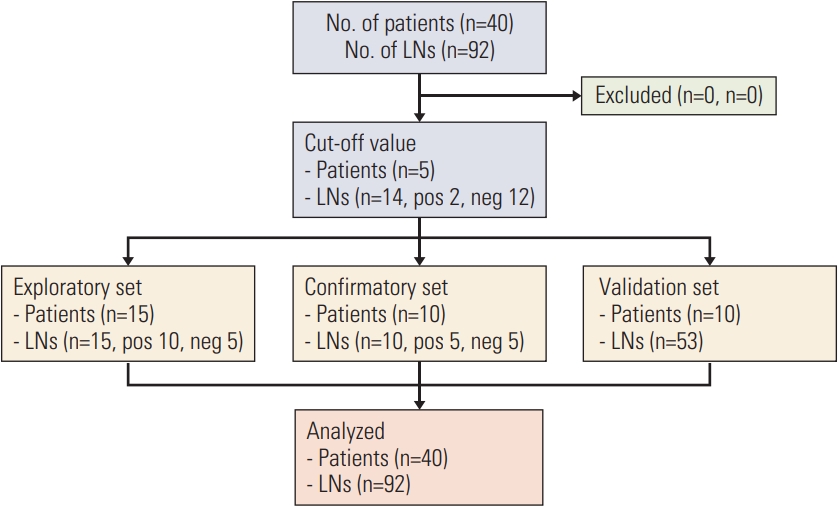
A total amount of 92 lymph nodes (52 SLNs, 40 non-SLNs) excised from 40 patients exhibiting breast cancer were harvested from the Breast Cancer Center of Kyungpook National University Chilgok Hospital between November 2015 and February 2016 (Fig. 1). The aggregate samples were then analyzed via RT-LAMP assay, direct RT-LAMP, and routine histopathology examination.
2. Primer design
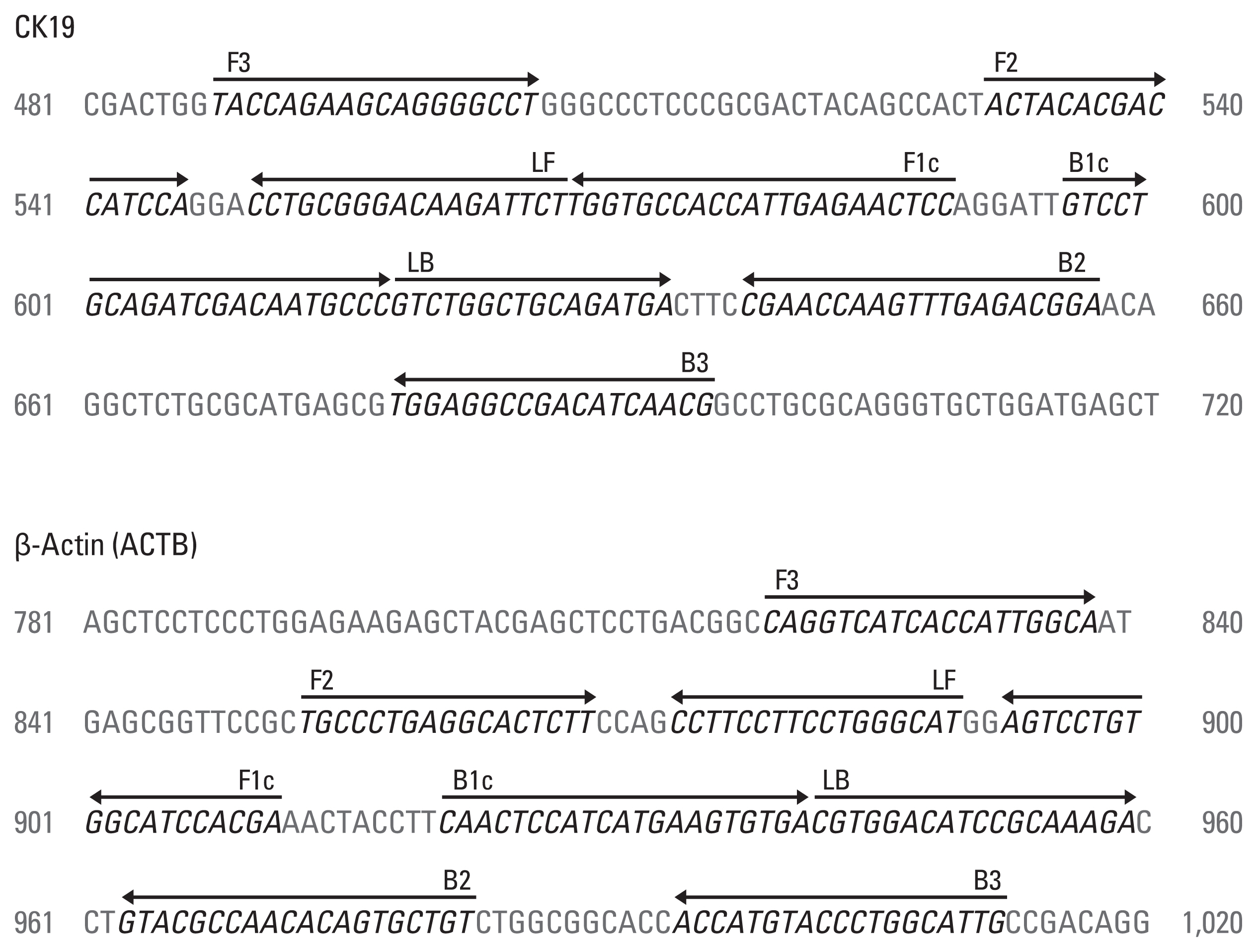
LAMP primers targeted at human CK19 were created between exons 1 and 3 in order to avoid cross-reactivity with sequences from pseudogenes utilizing Primer Explorer V4 (http://primereplorer.jp/elamp4.00/index.html). The RT-LAMP primer set is comprised of two outer (F3 and B3), two inner (FIP and BIP), and two loop (LF and LB) primers. To qualify and prove the integrity of isolated RNA, β-actin (ACTB) was additionally designed employing the same software. The sequences of each primer are displayed within Fig. 2.
3. RT-LAMP assays
RT-LAMP assays were carried out within a 25 μL reaction which included 12.5 μL of 2× reaction buffer (20 mM Tris-HCl pH 8.8, 10 mM KCl, 10 mM (NH4)2SO4, 8 mM MgSO4, 0.8 M betaine, 0.1% Tween 20, 1.4 mM dNTPs, 120 μM HNB), 1.5 μL of primer mixture (final concentration: 1.6 μM each of FIP and BIP, 0.2 μM each of F3 and B3, 0.8 μM each of LF and LB), 1 μL of enzyme mixture (16U Bst DNA polymerase and 120U M-MLV reverse transcriptase), 8 μL of DEPC-treated water, and 2 μL of the template RNA. DEPC-treated water was also employed for purposes of a negative control. The reaction mixture was conducted within a heating block (MaXtable H10, DAIHAN Scientific, Wonju, Korea) incubated at 58°C for 20 minutes and subsequently terminated at 80°C for 2 minutes. All of the experiments carried out were replicated three times. The positive reaction was indicated via a color alteration of the reaction buffer from the color pink to sky blue. The samples that became sky blue were counted as positive, while those that remained pink were counted as negative.
4. Determining cutoff values
A cutoff value for RT-LAMP assays between histopathologically positive and negative lymph nodes was determined utilizing 12 negative lymph nodes and two positive lymph nodes. Extractions of each RNA of lymph node (LN) was then diluted from 100 ng to 10 pg (100 ng, 1 ng, 100 pg, 10 pg). RT-LAMP assay was carried out utilizing the above concentration of RNA. The cutoff value was determined via the RNA concentration of the clinically metastasis-negative lymph nodes.
5. Direct RT-LAMP assay
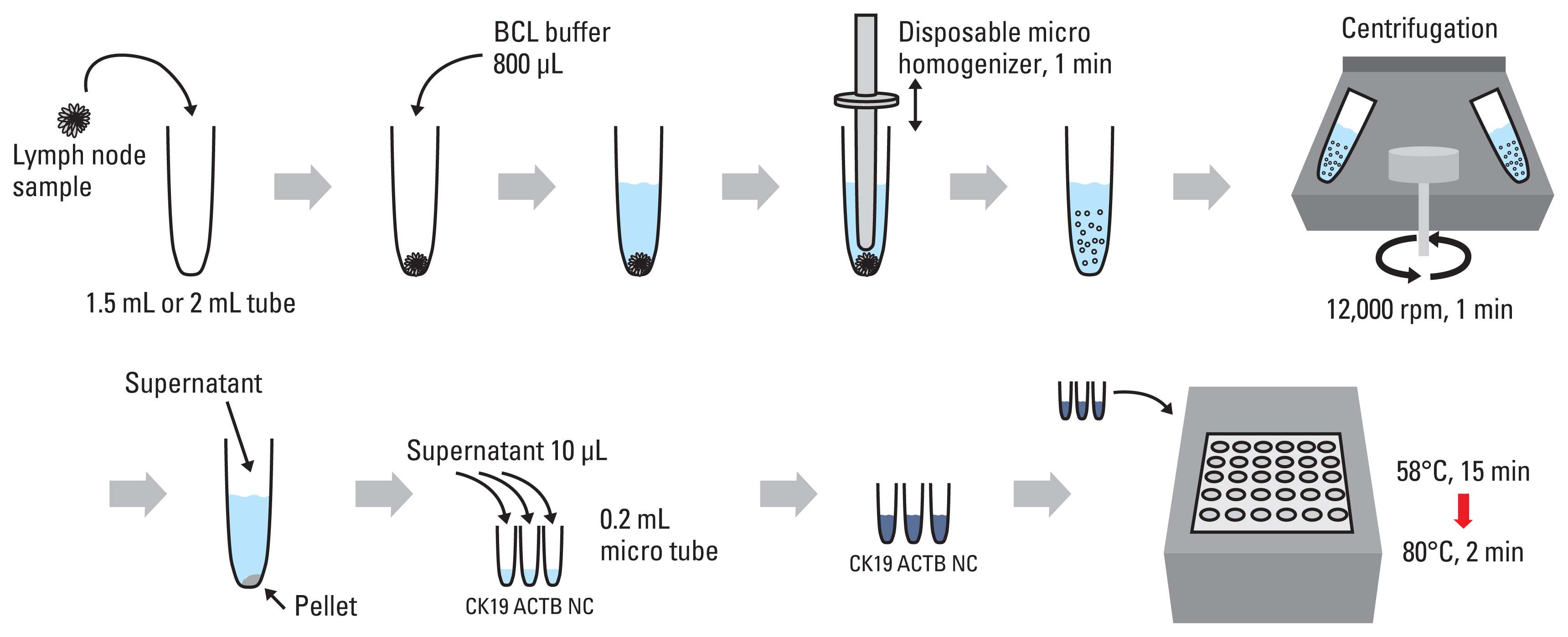
The lymph node tissue (2 mg < LN < 30 mg per reaction) was initially transferred into a 2 mL tube hosting 800 μL of BCL buffer (Mmonitor, Daegu, Korea). The SLN tissue was thus homogenized utilizing a disposable micro homogenizer (Takara, Tokyo, Japan) for a period of 1 minute and then was centrifuged at 12,000 rpm for a period of 1 minute. Following centrifugation, 10 μL lysate in place of DEPC water and an RNA template was employed for the direct RT-LAMP reaction. The reaction mixture is identical with RT-LAMP. The reaction was incubated at 58°C for 15 minutes and then terminated at 80°C for 2 minutes (Fig. 3). Direct RT-LAMP can be performed without prior RNA purification. The homogenization of lymph node with lysis buffer takes 5–10 minutes, and the reaction time of RT-LAMP is 25 minutes. Thus, the total reaction time of our direct RT-LAMP assay was 30–35 minutes.
6. Sensitivity of RT-LAMP assay
The breast adenocarcinoma MCF7 cell line was obtained from the Korean Cell Line Bank (Seoul, Korea). Cells were cultured within an RPMI1640 medium S1 Fig. with 10% FBS, 1% penicillin, and streptomycin (Gibco, Waltham, MA) at 37°C within a 5% CO2 atmosphere. The total RNA was extracted utilizing an RNeasy mini kit (Qiagen, Hilden, Germany) following the manufacturer’s protocol. The sensitivity of RT-LAMP was carried out using serially 10-fold diluted MCF7 cell line RNA from 100 ng to 1 pg as the template. The experiment was thus repeated in duplicate. The endpoint was calculated based upon the color change of the reaction buffer.
7. Exploratory test
For purposes of the exploratory set, clinically 10 positive and five negative nodes were surgically removed from the 15 patients exhibiting the early stage of breast cancer and then reviewed by two pathologists for conventional hematoxylin and eosin staining lacking any clinical information whatsoever. A single slice of 0.2 mm thickness sampled from each node were obtained during the frozen section procedure and sent to the laboratory for purposes of mRNA extraction and PCR for an innovatory diagnosis. Our team prospectively designed that, in case of 100% positive node metastasis via mRNA assay, another 10 positive and five negative nodes were thus sent to the lab for confirmation, which the lab was not made aware of.
Results
1. Patient characteristics
The clinicopathological features of the patients are displayed in Table 1. The median age of the patients comprised 51 years of age (range, 31 to 78 years), and the clinical stages of the cancer diagnosis prior to surgery were as follows: stage I (n=10, 25%), stage II (n=24, 60%), and stage III (n=6, 15%). Approximately 20% of the treated patients were administered NAC, 35 patients were subject to an SLN procedure, and 37 patients underwent ALND during the course of their surgical treatment. Invasive ductal carcinoma was the most frequent histologic type of cancer present (n=33, 82.5%); the majority of the tumors presented as estrogen receptor-positive (n=29, 72.5%) and half of the patients were grade 2 (n=23, 57.5%). Patients were staged following the guidelines of the 7th American Joint Committee on Cancer staging system.
2. Sensitivity of RT-LAMP
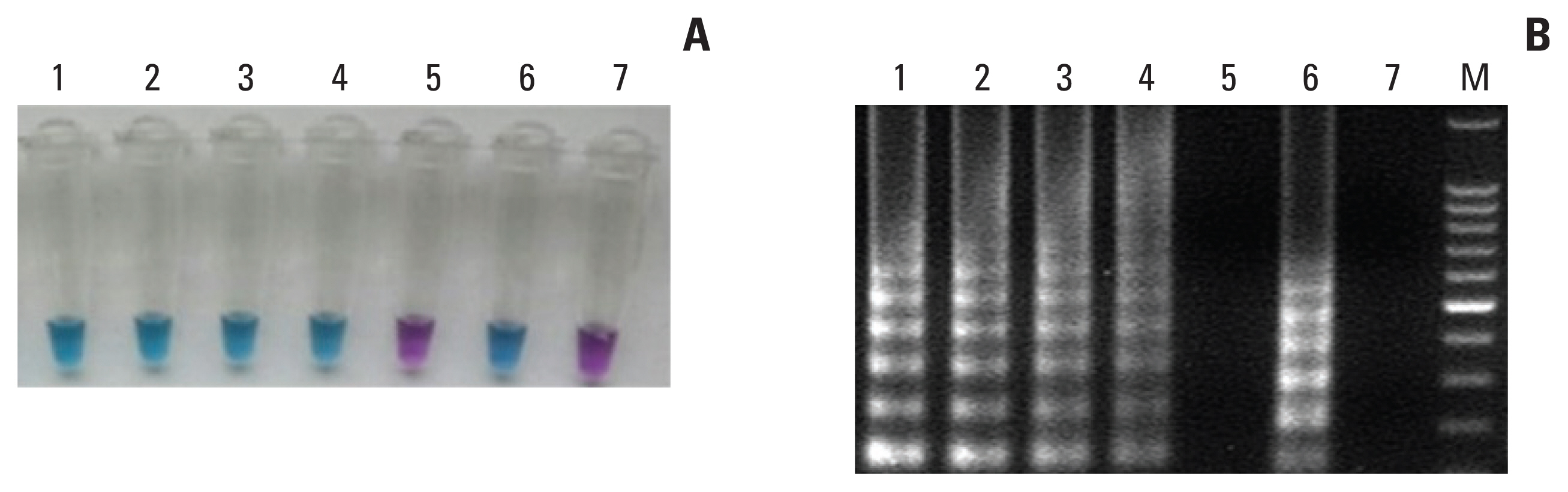
The sensitivity of RT-LAMP assay for detection of CK19 was calculated utilizing extracted total RNA from the MCF7 cell line. The RT-LAMP assay was able to amplify by 100 pg/μL of total RNA of MCF7 cell line. RT-LAMP products were additionally confirmed via 2% agarose gel electrophoresis (Fig. 4). The sensitivity of RT-LAMP assay for the detection of CK19 was 4 times higher than the previous result (12.5 pg vs. 50 pg).
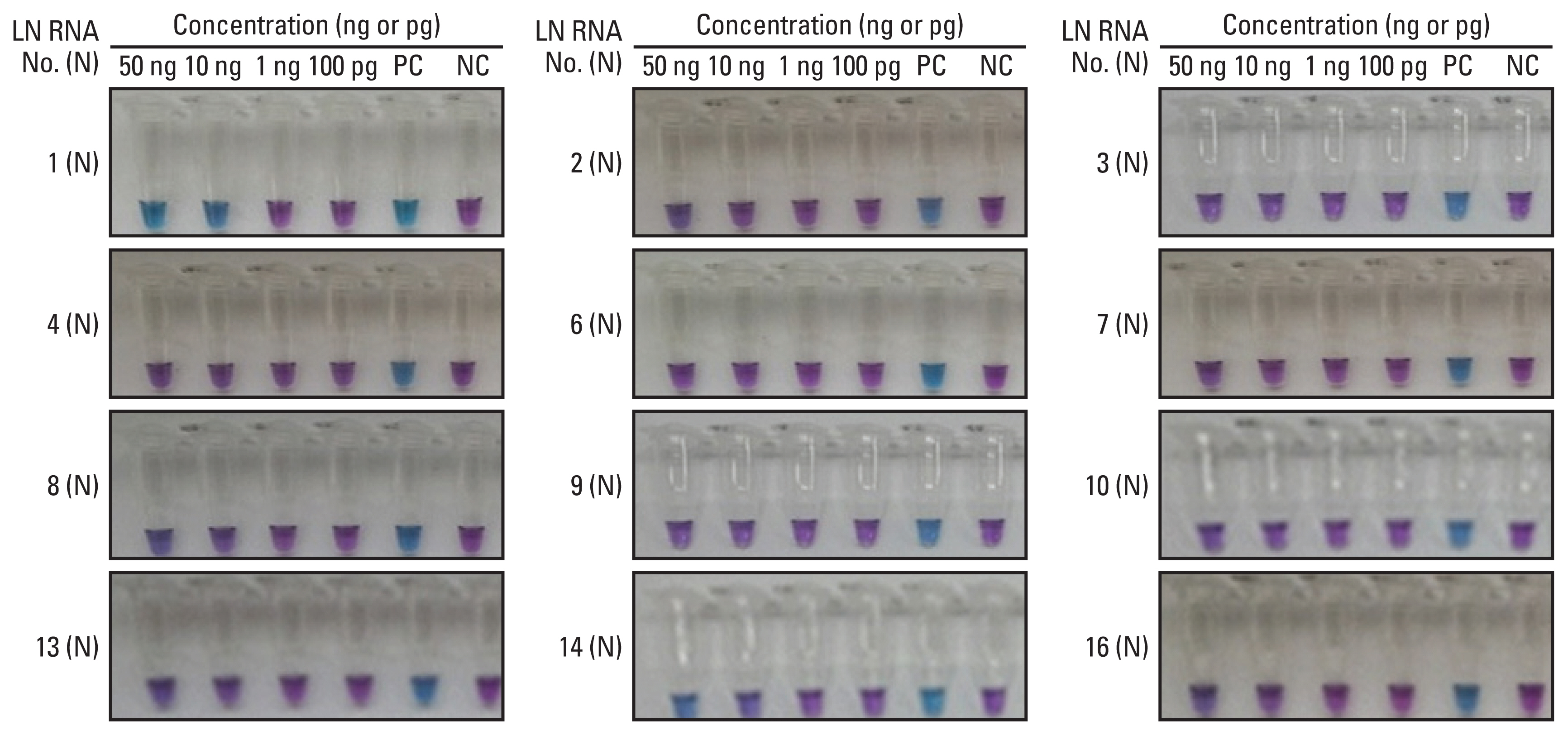
3. Cutoff value
A cutoff value for the RT-LAMP assay between the histopathologically positive and negative lymph nodes was calculated via the concentration of total RNA sampled from 12 negative LNs. To validate the cutoff value, our team analyzed total RNA concentration of positive LNs, which reveals the color change of reaction buffer. The concentration of total RNA from the histopathologically positive LNs was < 100 pg. Based on these results, our team established a cutoff value of 1 ng for distinguishing between metastasis-negative and -positive LNs. Using the cutoff value of 1 ng, we achieved 100% matched results between the RT-LAMP assay and histopathological examination (Fig. 5).
4. Performance of direct RT-LAMP relative to standard histology
Out of the 20 samples possessing histological metastases, 18 samples were direct RT-LAMP positive, yielding a sensitivity of 90%. Of the 25 histology-negative samples, 25 possessed negative direct RT-LAMP results, yielding a specificity of 100%. The positive predictive value and negative predictive value were 100% and 92.6%, respectively (Table 2).
Discussion
In the present study, our team analyzed the performance of direct RT-LAMP assay utilizing heat-treated samples lacking RNA extraction. The sensitivity and specificity of the direct RT-LAMP assay were 85.7% and 100%, respectively. The positive predictive value and negative predictive value were 100% and 94.4%, respectively.
Various previous studies analyzed the performance of RT-LAMP for the purposes of detection of SLN metastases within breast cancer patients [7–9]. Szychta et al. [7] revealed 100 % of sensitivity and 90.47 % of specificity for the RT-LAMP method to intraoperative detection of LN metastasis across 98 breast cancer patients. Furthermore, Cserni [10] demonstrated the various results of histological and RT-LAMP tests in varying validation series. They demonstrated levels of 91%–100% of sensitivity and 93.4%–99.3% of specificity for each study. Previous meta-analysis revealed the pooled sensitivity, specificity, and area under the summary receiver-operating characteristic curve (AUC) for overall metastasis were 0.90, 0.96, and 0.98, respectively [11]. In our study, we demonstrated that comparable sensitivity and specificity of the direct RT-LAMP assay for detection of lymph node metastasis in breast cancer patients (90% and 100%, respectively).
A direct RT-LAMP assay utilizing heat-treated samples lacking RNA extraction was first developed and evaluated for the detection of specific virus (EV71 subgenotype C4) within nasopharyngeal swab specimens [12]. The sensitivity and specificity was reported to be 90.3% and 100%, respectively, as compared to RT-LAMP, and 86.3% and 100% respectively, as compared to quantitative real-time PCR. Recently, Mohon et al. developed a direct RT-LAMP method targeting 20 genes encoding the spike (S) protein and RNA-dependent RNA polymerase of severe acute respiratory syndrome coronavirus 2. They revealed that the direct RT-LAMP assay achieves a comparable limit of detection for commonly utilized RT-PCR protocols [13]. However, few studies exist evaluating LN metastasis within breast cancer patients utilizing a direct RT-LAMP method. In the present study, our team applied a direct RT-LAMP assay in order to detect LN metastasis within breast cancer patients.
Even though, the performance of former RT-LAMP for detection of SLN in breast cancer patients is quite good, the RNA extraction step requires approximately 30 minutes, the omission of RNA extraction could possibly save both time and labor for the preparation of the samples for RT-LAMP [14]. Direct RT-LAMP can be performed without prior RNA purification. Thus, the total reaction time of our direct RT-LAMP assay was 30–35 minutes.
Furthermore, the performance of direct RT-LAMP for the detection of LN metastasis is strong enough to replace standard histology. Previous studies reported that the intraoperative frozen section SLN examination has only 50% to 70% sensitivity for the detection of metastasis compared with the permanent histologic section of the permanent histologic sections [15]. Besides, complete analysis of the sentinel lymph node biopsy specimen requires extensive preparation and time-consuming reviews [16].
However, some limitations should be noted. First, the direct RT-LAMP assay is not a quantitative method and cannot be used to predict the size of the metastasis. Second, the sample size was limited.
In conclusion, the direct RT-LAMP is a new and reliable method for the molecular staging of lymphatic metastasis within breast cancer. The results showed the potential clinical feasibility of direct RT-LAMP as a useful diagnostic tool for detecting LN metastasis with high sensitivity and specificity. Further large-scale studies are necessary in order to determine the clinical utility of this method.