Introduction
Immune checkpoint inhibitors (ICIs) have opened a new era of cancer management through the leverage of the immune system’s potential and have become one of the mainstays of antitumor treatment [1]. The activation and proliferation of T cells are modulated by certain inhibitory surface signaling molecules, so-called checkpoints. Several different immune checkpoint molecules have been identified, in particular, cytotoxic T-lymphocyte antigen 4 (CTLA-4) and programmed cell death protein 1 (PD-1) and its ligand 1 (PD-L1). Selectively blocking the interaction of ligands with these checkpoints can lead to amplification of T cell–mediated immunity and disruption of tumor immune escape. Substantial clinical studies have demonstrated that antibodies against CTLA-4 and PD-1/PD-L1 can yield a significant survival improvement in several tumor types, including metastatic melanoma, non-small cell lung cancer, and renal cell carcinoma [2–5]. However, the routine application of these novel ICI drugs highlights the essence of knowledge and management of ICI-induced immune-related adverse events (irAEs).
In light of the fact that ICI delivers positive antitumor efficacy by interfering with immune system regulation, an activated immune response might attack normal body tissues and be responsible for the development of irAEs. The common irAEs include colitis, hepatitis, pneumonitis, nephritis, and endocrinopathies [6,7]. Although the majority of irAEs show moderate toxicity, there have been reports of ICI- induced deaths, mainly due to autoimmune colitis, myocarditis, and myasthenia gravis [2,8–11]. Most of mild-to-moderate irAEs can be well controlled by observation and supportive treatment without withholding ICI drugs, however, patients with severe irAEs still require enhanced and timely medical interventions, such as corticosteroids and immunosuppressive agents, in line with the guidelines of the National Comprehensive Cancer Network (NCCN) and European Society for Medical Oncology (ESMO) [12,13]. Our previous study revealed that the toxicity profile and incidence of irAEs varied among ICI drugs [14]. However, the pattern of the time to onset and resolution of ICI-induced irAEs remains undetermined and is worth further exploration. There are few studies concerning the pattern of irAE development in cancer. Martins et al. [15] proposed that the majority of grade ≥ 3 irAEs induced by anti–CTLA-4 antibodies occur within 8–12 weeks of commencing treatment. Skin rash usually had the earliest onset and irAEs tended to occur earlier in the course of nivolumab (NIV) plus ipilimumab (IPI) treatment than in that of IPI monotherapy [15]. Nonetheless, the results were summarized through a literature review rather than statistical calculations and the time to resolution was not investigated. Although Weber et al. [16] demonstrated a characteristic pattern of the occurrence of irAEs, these results were generated based on small sample size (n=325) and the pattern was applicable to only four organ-specific irAEs and specific treatment of IPI 10 mg/kg every 3 weeks, failing to provide a comprehensive view of ICI-induced irAEs in pan-cancers [16].
By using the data derived from robust clinical trials, we conducted a pooled analysis to investigate the pattern of the time to onset, resolution, and immune-modulation resolution of irAEs in cancer, intending to aid a better understanding, timely detection, and effective management of ICI-induced irAEs in routine practice.
Materials and Methods
A prospective protocol was created and uploaded to the PROSPERO online platform, with the registration number CRD42020167835.
1. Data sources and searches
We searched for relevant studies published between January 2007 and December 2019 through public electronic databases, including PubMed, Embase, Cochrane Library, and Web of Science. Two investigators (S.Q.T. and C.X.) determined the final search strategy (Supplementary Materials). After screening the titles or abstracts, full texts were assessed, and references of relevant publications were manually searched.
2. Study selection
We included phase II–III clinical trials that reported the median time to onset, resolution, or immune-modulation resolution of irAEs in cancer receiving ICI-based treatments (e.g., ICI alone or ICI plus conventional therapy). Conventional therapies (CT) included chemotherapy, radiotherapy, and so on. The definitions for outcomes above were listed in Supplementary Materials and were consistent among all included clinical trials. We excluded conference abstracts and presentations of ongoing clinical trials due to the insufficient information.
3. Data extraction and processing
We extracted the data from the main text and supplementary materials. Two reviewers (S.Q.T. and C.X.) independently recorded the data on a predesigned list (Supplementary Materials). Data from the updated study were used to supplement those from the previous report of the same trial. Common Terminology Criteria for Adverse Events were used to evaluate the adverse events and grade the severity of each irAE [17]. Grade ≥ 3 irAEs were considered severe events.
4. Quality assessment
Two reviewers (S.Q.T. and C.X.) used the tool recommended by the Cochrane Collaboration Handbook and the modified Jadad scale to evaluate the quality of the included clinical trials [18,19]. Discrepancies regarding study selection, data extraction, and quality assessment between two reviewers were resolved by discussion.
5. Data synthesis and statistical analysis
The timing data that represented different event subsets to the same organ-specific irAEs were pooled as the timing data of that category. For example, the time to onset of hyperthyroidism and hypothyroidism would be pooled as that of endocrine events. The data with censored values were excluded. We used the pooled median time (weighted median time) to onset (PMT-O), resolution (PMT-R), and immune-modulation resolution (PMT-IMR) and their 95% confidence interval as summary statistics. The outcomes were generated by using the metamedian package in R ver. 3.6.1 (http://www.r-project.org/) [20]. The primary outcomes were PMT-O and PMT-R of all-grade irAEs. The secondary outcomes were PMT-IMR of all-grade irAEs and the outcomes of grade ≥ 3 irAEs. All outcomes were assessed from two different perspectives: overview and detail, based on the time of development of all irAEs and that of organ-specific irAE, respectively.
Given that the different toxicity profiles among ICI agents, the PMT-O, PMT-R, and PMT-IMR were compared between PD-1/PD-L1 inhibitor, CTLA-4 inhibitor, and combination therapy (i.e. more than one kind of ICI agent). The former two treatments refer to applying one ICI agent with or without CT. Subgroup analyses were based on ICI drugs, ICI doses, and cancer types.
Data visualization methods were used to depict the pooled median time and 95% confidence interval via Microsoft Excel (Microsoft, Inc., Redmond, WA). We used the Z test to identify the differences among PMT-O, PMT-R, and PMT-IMR by SPSS ver. 24.0 (IBM Corp., Armonk, NY). All p-values were two-sided with significance defined as p < 0.05.
Results
1. Literature search and characteristics
We included 22 studies involving 23 clinical trials and 8,436 patients in this study (S1 Table, S2 Fig.) [3,21–41]. The baseline characteristics of each study were shown in Table 1. Thirteen clinical trials (56.5%) were phase III trials. One study reported the pooled results of a phase I and a phase II clinical trial with a large sample size of 1,738 patients; thus, the phase I trial was also included [32]. The cancer types included lung cancer (number of the involving trials=6), melanoma (n=7), urinary system cancer (n=4), and other (n=6). PD-1/PD-L1 blockade-based treatments included monotherapy of NIV (n=10), pembrolizumab (n=2), and avelumab (n=2). CTLA-4 blockade-based treatments included IPI monotherapy (n=5) and IPI+CT (n=3). Combination therapy included NIV+IPI (n=5). Subgroup analysis included two updated clinical trials without duplicate counting of their sample sizes [30]. According to modified Jadad scores, 20 studies were assessed as high quality, and two studies were assessed as relatively low quality (S3 Table) [3,23].
2. Pooled analysis of the time to onset
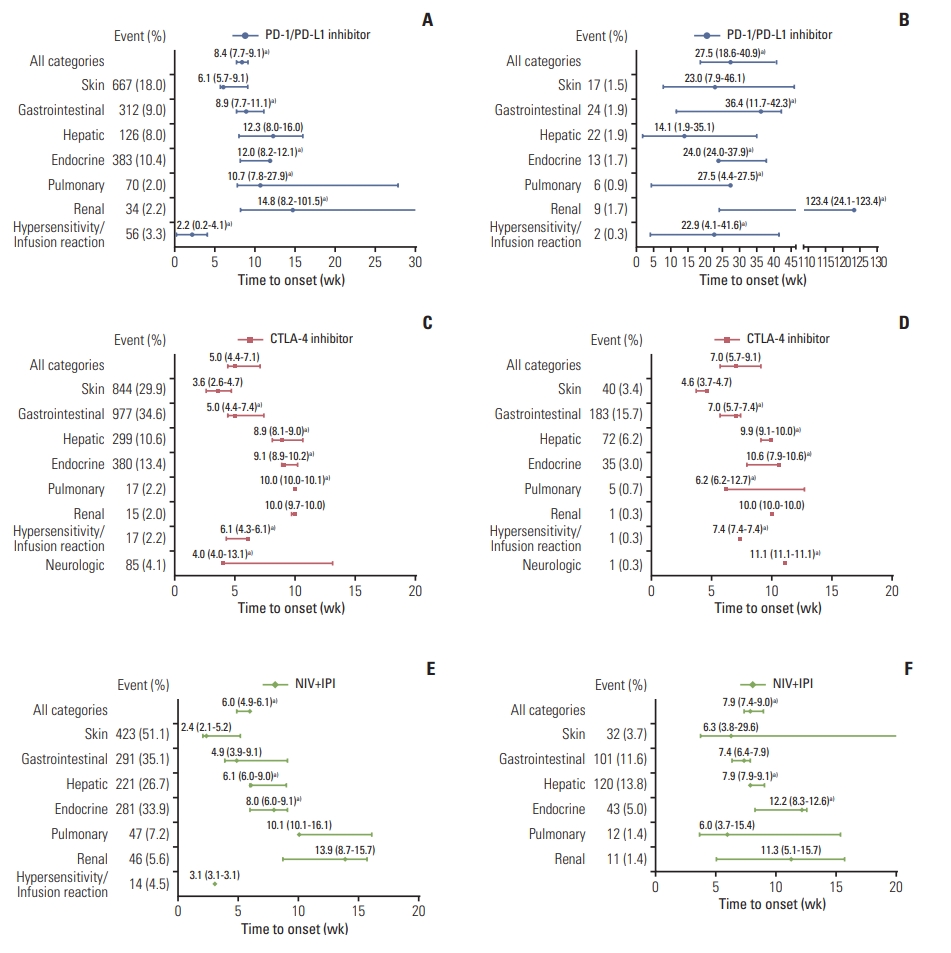
The PMT-O of all-grade irAEs ranged from 2.2 to 14.8 weeks. The four irAEs with the top shortest PMT-O were skin, hypersensitivity/infusion reaction, gastrointestinal, and neurologic events, while the longest PMT-O was observed in renal events (Fig. 1A, C, and E).
The PMT-O of grade ≥ 3 irAEs ranged from 4.6 to 12.2 weeks for CTLA-4 inhibitors and NIV+IPI treatment and ranged from 14.1 to 123.4 weeks for PD-1/PD-L1 inhibitors. Compared with all-grade irAEs, the PMT-O of grade ≥ 3 irAEs was significantly longer for PD-1/PD-L1 inhibitors (27.5 weeks vs. 8.4 weeks, p < 0.001) and NIV+IPI treatment (7.9 weeks vs. 6.0 weeks, p < 0.001) in overview; as for CTLA-4 inhibitors, that was significantly longer in gastrointestinal (7.0 weeks vs. 5.0 weeks, p=0.023), hepatic (9.9 weeks vs. 8.9 weeks, p=0.002), endocrine (10.6 weeks vs. 9.1 weeks, p=0.049), hypersensitivity/infusion reaction (7.4 weeks vs. 6.1 weeks, p=0.005), and neurologic events (11.1 weeks vs. 4.0 weeks, p=0.002) (Fig. 1).
3. Pooled analysis of the time to resolution
The PMT-R of all-grade irAEs ranged from 0.1 to 54.3 weeks. The five irAEs with the top shortest PMT-R were hypersensitivity/infusion reaction, gastrointestinal, pulmonary, hepatic, and renal events, which might be resolved within 10.5 weeks (Fig. 2A, E, and I). The PMT-R of grade ≥ 3 irAEs was within 7.9 weeks when excluding endocrine events (Fig. 2B, F, and J).
In overview, the PMT-R was comparable between grade ≥ 3 and all-grade irAEs. By organ, the PMT-R of grade ≥ 3 irAEs was significantly shorter than that of all-grade irAEs induced by NIV+IPI treatment in skin (3.1 weeks vs. 10.9 weeks, p=0.049), endocrine (11.6 weeks vs. 27.6 weeks, p < 0.001), pulmonary (1.5 weeks vs. 4.5 weeks, p=0.010), and renal events (2.4 weeks vs. 6.3 weeks, p=0.028) (Fig. 2A, B, E, F, I, J). When applying the immune-modulation drug, the time to resolution of grade ≥ 3 irAEs was significantly shorter than that of all-grade irAEs caused by PD-1/PD-L1 blockade (6.9 weeks vs. 40.6 weeks, p=0.002) and NIV+IPI treatment (3.1 weeks vs. 5.9 weeks, p=0.031) in the overview. As for CTLA-4 blockade, the PMT-IMR of grade ≥ 3 irAEs was significantly shorter than that of all-grade irAEs in skin (8.5 weeks vs. 14.4 weeks, p < 0.001), gastrointestinal (3.3 weeks vs. 4.4 weeks, p < 0.001), and hypersensitivity/infusion reaction (0.3 weeks vs. 2.1 weeks, p < 0.001) (Fig. 2C, D, G, H, K, and L).
When compared with PMT-R, the PMT-IMR of all-grade irAEs caused by PD-1/PD-L1 inhibitors was significantly longer (40.6 weeks vs. 10.1 weeks, p=0.010) in overview; as for CTLA-4 inhibitors, the PMT-IMR was significantly longer in skin (14.4 weeks vs. 9.3 weeks, p=0.004), gastrointestinal (4.4 weeks vs. 2.9 weeks, p < 0.001), and hypersensitivity/infusion reaction (2.1 weeks vs. 0.1 weeks, p < 0.001) (Fig. 2A, C, E, G, I, and K). Regardless of grading, hypersensitivity/infusion reaction and endocrine events were associated with the shortest and longest PMT-IMR, respectively, which were similar to the patterns of PMT-R.
4. Subgroup analysis based on ICI drugs
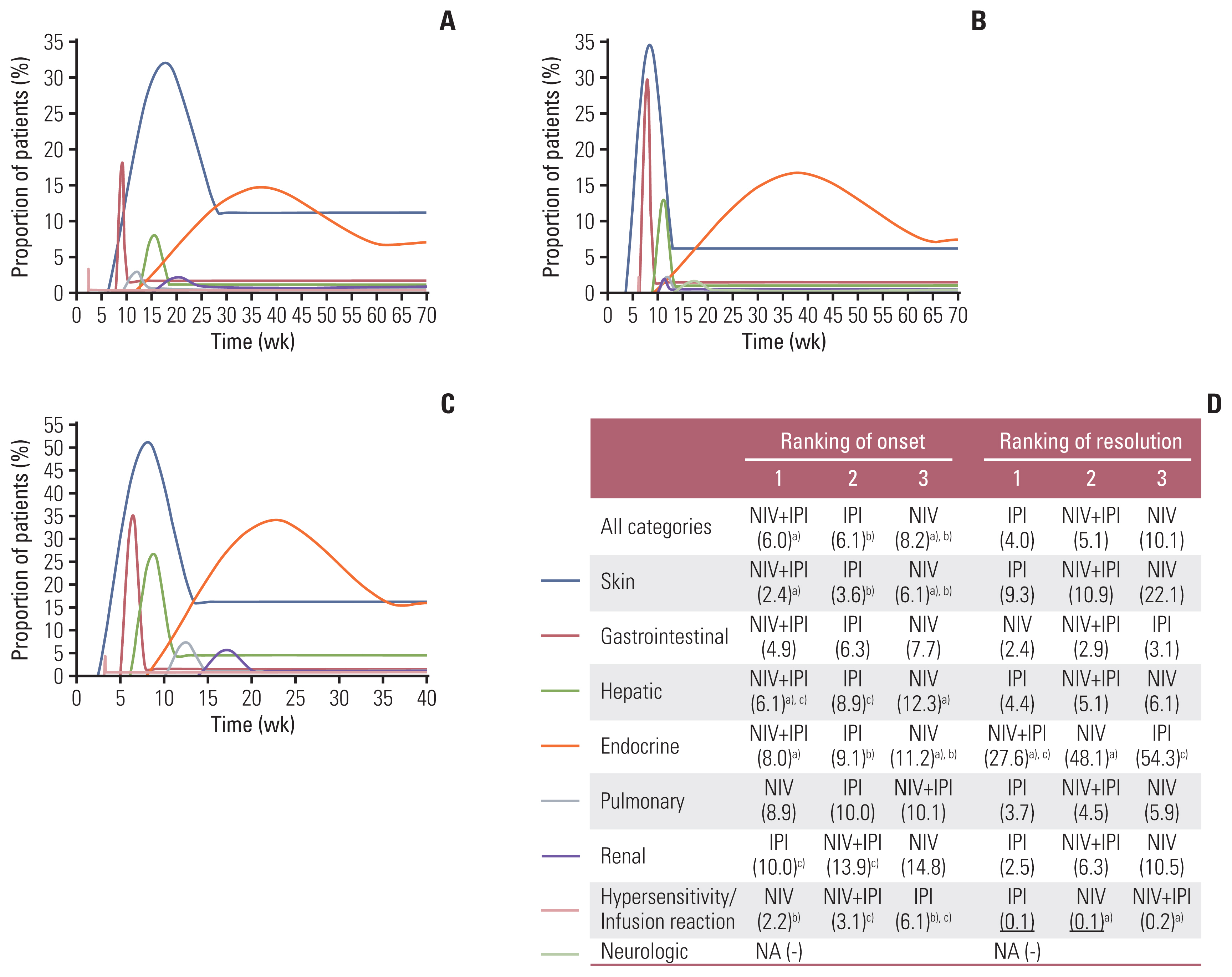
NIV monotherapy was associated with significantly longer PMT-O of all-grade irAEs than NIV+IPI (8.2 weeks vs. 6.0 weeks, p < 0.001) and IPI alone (8.2 weeks vs. 6.1 weeks, p=0.012). The PMT-R was comparable between NIV+IPI and the corresponding monotherapy (Fig. 3).
In terms of grade ≥ 3 irAEs, NIV monotherapy had the significantly longest PMT-O among these three treatments in overview (IPI vs. NIV+IPI vs. NIV: 7.4 weeks vs. 7.9 vs. 27.5 weeks; p < 0.05), especially in gastrointestinal (7.0 weeks vs. 7.4 weeks vs. 36.4 weeks, p < 0.001), endocrine (10.6 weeks vs. 12.2 weeks vs. 24.0 weeks, p < 0.05), pulmonary (6.2 weeks vs. 6.0 weeks vs. 27.5 weeks, p < 0.05), and renal events (10.0 weeks vs. 11.3 weeks vs. 123.4 weeks, p < 0.001) (S4 Table).
In overview, the PMT-O and PMT-R were comparable between IPI alone and IPI+CT. By organ, the PMT-O of hepa-tic (8.9 weeks vs. 5.9 weeks, p < 0.001) and neurologic events (13.1 weeks vs. 4.0 weeks, p < 0.001) and the PMT-R of skin (9.3 weeks vs. 4.3 weeks, p=0.037) and endocrine events (54.3 weeks vs. 10.4 weeks, p < 0.001) were significantly longer in IPI cohort than in IPI+CT cohort (S5 Fig.).
5. Subgroup analysis based on ICI dose
The PMT-O and PMT-R were similar between the two different doses of IPI, except for those of endocrine events and PMT-O of neurologic events. Compared with NIV 1 mg/kg every 3 weeks and IPI 3 mg/kg every 3 weeks, significantly longer PMT-O of skin (5.1 weeks vs. 2.1 weeks, p < 0.001), hepatic (9.0 weeks vs. 6.0 weeks, p < 0.001), pulmonary (15.4 weeks vs. 10.1 weeks, p < 0.001), and renal events (15.7 weeks vs. 13.9 weeks, p=0.002) were observed in the treatment of NIV 3 mg/kg every 3 weeks and IPI 1 mg/kg every 3 weeks; the PMT-R was comparable between two doses of combination therapy in all events except for the gastrointestinal irAE (Table 2).
6. Subgroup analysis based on cancer type
The PMT-O of all-grade irAEs was significantly shorter in lung cancer cohort than in melanoma cohort (4.7 weeks vs. 6.1 weeks, p=0.017), including renal (8.2 weeks vs. 13.9 weeks, p=0.048), hypersensitivity/infusion reaction (0.2 weeks vs. 3.3 weeks, p=0.004), and neurologic (4.0 weeks vs. 13.1 weeks, p < 0.001) events (Table 3). Under the treatment of NIV 3 mg/kg every 2 weeks, two groups showed significantly different PMT-O of hepatic (lung cancer vs. melanoma: 8.0 weeks vs. 14.1 weeks, p < 0.001), hypersensitivity/infusion reaction (0.2 weeks vs. 3.3 weeks, p < 0.001), endocrine (11.2 weeks vs. 8.2 weeks, p=0.007), and pulmonary events (27.9 weeks vs. 8.7 weeks, p=0.001). The PMT-R of organ-specific irAEs were comparable between the two cancer types, except for that of skin events (S6 Table).
Discussion
Currently, ICI is considered to be a promising treatment option for patients with cancer. However, the adverse events associated with immunologic etiology cannot be ignored. Although substantial evidence has demonstrated the safety profile of ICIs, most studies have focused on the incidence and certain kinds of ICI drugs, and the typical timing of the development of irAEs remains unclear [42–46]. In this study, we aim to clarify the pattern of time to onset and resolution of ICI-induced irAEs in pan-cancers; therefore, it can provide clues for early recognition and timely management of irAEs to clinicians.
The premise of the successful management of irAEs and the reduction of sequelae is mastering the general pattern. In the previous studies of patients with melanoma receiving ICI monotherapy, it was reported that skin-related irAE was the earliest event to appear (median, 2–6 weeks), followed by gastrointestinal events (6–7 weeks), while renal events were the last to appear (15 weeks). Moreover, endocrine irAEs was the last (28 weeks) event to be resolved [3,16]. The pattern reported in our study was consistent with the above findings. Apart from the commonly selected irAEs in previous studies, we also included hypersensitivity/infusion reaction and neurological events in the analysis, and the former was newly found to be the first to resolve.
Severe irAEs were prone to occur later and be resolved with immune-modulation agents earlier than mild-to-moderate irAEs. On the one hand, this result may be due to the dose-dependent effect of irAEs. In a phase II trial comparing three dose administration of IPI (0.3 mg/kg, 3.0 mg/kg, and 10 mg/kg) in patients with advanced melanoma, the incidence of irAEs was 26%, 56%, and 70% and occurrence of grade 3–4 irAEs was 0%, 7%, and 25% of patients, respectively [47]. Similarly, a dose-based network meta-analysis suggested that high-dose IPI had a greater incidence of 3–4 grade irAEs than low-dose IPI [14]. Besides, in a phase I trial assessing the safety of anti–PD-1 antibody in patients with multiple cancer, an increase in the frequency of grade 3–4 irAE (0%, 4%, and 8%) was observed with an increasing dose level (0.3 mg/kg, 3.0 mg/kg, and 10 mg/kg, respectively) [48]. ICI drugs reach a higher cumulative dose in the later treatment course, therefore inducing late-onset severe irAEs. On the other hand, positive clinical management might foster the earlier resolution of severe irAEs. According to the NCCN and ESMO clinical practice guidelines for the management of immunotherapy-related toxicities, the common management would be observation and supportive treatment when initially encountered with grade 1–2 irAEs [12,13]. However, enhanced medical interventions and close nursing care will be adopted on the condition of dealing with severe irAEs. Given that ICI is a novel therapy with high hopes in the current spotlight, clinicians are more likely to find severe irAEs and perform timely resolutions.
The endocrine-related irAEs featured delayed onset (8.0–12.0 weeks), the longest resolution duration, and the lowest resolution rate in all ICI regimens. This result corroborates those from a study investigating IPI, where it took 9 weeks before the onset of endocrine events [16]. The underlying reason for the long time to recover from endocrine-related irAE was that it might take time for patients to become adequately replaced with the exogenous hormone. Thus, closer follow-up is needed approximately 9 weeks after the start of treatment, and patients should be provided with appropriate education regarding this prolonged treatment, including guidelines for psychological construction, medication norms, regular follow-up time, and adjustment of drug dose.
The irAEs caused by NIV+IPI generally occurred earlier than those induced by NIV alone. In a review, irAEs tended to occur earlier in the course of treatment with IPI plus an anti–PD-1 antibody compared with IPI monotherapy or anti–PD-1/(PD-L1) antibodies [15]. Similarly, a study of 1,551 patients assessed by the European Medicines Agency demonstrated that most of the irAEs occurred earlier in the NIV+IPI cohort than in the monotherapy cohort, including skin, gastrointestinal, hepatic, endocrine and renal events [49].
Although irAEs generally occurred within 14.8 weeks after the first dose of ICI drugs, they could appear several months even years after the completion of treatment. In this study, we noticed that the maximum time to onset could reach three years after starting treatment in some cases. The wide range in time of onset was also described in recent publications. The cutaneous presentation occurred in patients up to 60 weeks after the first dose of anti–PD-1 treatment in stage IV melanoma [50]. Ocular adverse effects were experienced by some patients with metastatic melanoma 1 year after the last dose of IPI [51]. Although the half-life of ICI is ascertained, such as two weeks for IPI, it may still have a biological effect for a long time after the drug is cleared [13,52]. Thus, surveillance should be reinforced and a long-term multidisciplinary follow-up should be arranged.
Several limitations should be mentioned. First, irAEs were diagnosed by investigators, which might be influenced by clinical experience. Indeed, the incidence of irAEs reported by randomized controlled trials published after 2017 seemed greater than those before (76.9% vs. 58.5%). It may be because more attention has been paid to these adverse events and more clinical experience has been gained. Hence, the quantifiable criteria to clarify the definition of irAE are eagerly awaited. Second, standard deviations or quartile information of timing data were not extracted and analyzed because they were rarely reported. Nevertheless, to make a reliable estimation, the metamedian method used in this study was proved to be well-performed under this circumstance by collecting median values [20]. Third, the dataset of the group receiving anti–PD-1/PD-L1 treatment mainly originated from the trials on NIV. Thus, the applicability of corresponding results may be more specific to NIV monotherapy and the clinical trials involving ICI agents are recommended to report the time data on the development of irAEs in the future. Fourth, the subgroup analysis of cancer types involved a small number of trials, so the relevant results should be regarded with caution.
The irAEs induced by ICI agents appear to be an emerging challenge in clinical practice. This study revealed the occurrence pattern of irAEs, expanding the knowledge of the characteristics of this new issue. Our findings may serve as a useful tool to help clinicians detect irAEs timely and make therapeutic decisions properly.