Introduction
Non-Hodgkin lymphoma (NHL) represents a heterogeneous group of malignancies with distinct clinical and pathological features. New treatments have improved the outcomes of NHL, but a substantial number of patients still relapse and require multiple treatments because only a limited number of patients respond to salvage treatment and the response is usually of short duration [1,2]. Furthermore, as intensified salvage chemotherapy is repeated, treatment-related toxicity contributes to long-term morbidity and poor survival outcomes. Thus, there is an unmet need for more effective and less toxic drugs for the treatment of NHL. Recent improvements in the understanding of the evasion of the immune response by tumor cells have led to the identification of immune checkpoint inhibition as a new tool for cancer treatment [3]. The programmed cell death protein 1 (PD1) is an immune checkpoint that regulates the host immune response. The binding of PD1 ligand 1 (PDL1) on tumor cells to PD1 on the surface of effector T-cells transduces inhibitory signals to the T cells, allowing tumor cells to escape antitumor immunity [4]. Therefore, inhibition of this interplay between PD1 and PDL1 can reverse this immune escape and enhance T-cell cytotoxicity against tumor cells. Currently, two monoclonal IgG4 anti-PD1 antibodies, nivolumab and pembrolizumab, are approved by the Food and Drug Administration (FDA) as salvage treatment for solid cancers such as melanoma and non-small cell lung cancer. The FDA has also granted accelerated approval to nivolumab and pembrolizumab for the treatment of relapsed or refractory classical Hodgkin lymphoma (HL). However, data concerning the use of pembrolizumab in patients with NHL are limited because its efficacy in relapsed or refractory NHL has not been determined. In our institute, we have used pembrolizumab to treat patients with various subtypes of relapsed or refractory NHL, and already reported the exciting outcome of one patient with relapsed NK/T-cell lymphoma (NKTCL) in a previous multicenter retrospective study [5]. Since January 2016, we have used pembrolizumab as a salvage treatment for thirty patients with relapsed or refractory NHL. In this study, we retrospectively analyzed their treatment outcome to illustrate our real-world experience with pembrolizumab treatment in relapsed or refractory NHL outside of clinical trials.
Materials and Methods
1. Patients and treatment
Thirty consecutive patients with relapsed or refractory NHL were treated with pembrolizumab at the Samsung Medical Center between January 2016 and September 2017. Informed consent for the use of pembrolizumab was obtained from all patients. Because the cost of pembrolizumab is not reimbursed by health insurance in Korea, a fixed low dose of 100 mg was administered to 27 patients while three patients received the recommended dose of 200 mg. The treatment cycle was repeated every 3 weeks. The response was assessed using 2-deoxy-2-fluorine-18-fluoro-D-glucose positron emission tomography integrated with computed tomography and computed tomography according to standard criteria. In most patients, the first response evaluation was performed after the second or third cycle of treatment [6]. If signs of rapid deterioration were observed, response evaluation was performed earlier than the planned date. For patients with NKTCL, blood Epstein–Barr virus (EBV) DNA titer was also quantified as previously reported as an indirect biomarker of the extent of disease [7].
2. Assessment of PDL1 expression in NHL
We assessed PDL1 expression of tumor cells by immunohistochemistry (IHC) to evaluate the extent of PDL1 expression in various subtypes of NHL. Thus, PDL1 expression was assessed in relapsed or refractory NHL patients (n=76) for whom paraffin-embedded tissue blocks were available for IHC. Most tissue samples were from archived tissue samples in our lymphoma registry that were obtained as routine clinical practice at the time of diagnosis (n=71), and only five cases were from obtained at relapse or progression. After IHC, we analyzed the proportion of cells in each tumor subtype that expressed PDL1 to determine whether PDL1 expression differed according to subtype of NHL. We also evaluated the EBV positivity of tumor cells, correlating the results of EBV in situ hybridization with PDL1 expression for each subtype of NHL. These 76 patients included 21 patients treated with pembrolizumab who were analyzed for response evaluation. Thus, we could evaluate the PDL1 expression of tumor cells in patients receiving pembrolizu-mab to determine whether the response to pembrolizumab was correlated with PDL1 expression.
3. IHC for PDL1 and EBV positivity
Two assays including monoclonal antibodies against PDL1 were used: the Ventana PDL1 (SP142) assay (1:25, rabbit antihuman PDL1/CD274 monoclonal antibody, clone SP142, Ventana, Tucson, AZ) and the PDL1 IHC 22C3 pharmDx assay, which includes the murine 22C3 anti-human PDL1 antibody (Dako, Carpinteria, CA). PDL1 IHC using the Ventana PDL1 assay was performed on an automated immunostainer (Benchmark, Ventana) according to the manufacturer’s instructions. In some cases, PDL1 IHC was performed using the PDL1 IHC 22C3 pharmDx kit using a Link 48 autostainer according to the manufacturer’s instructions. Because it was difficult to identify tumor cells precisely when observing only hematoxylin and eosin (H&E) stained slides, PDL1 expression on tumor cells was investigated by comparing H&E slides. The proportion of PDL1-positive cells was estimated as a percentage of total tumor cells; tumor cells typically showed membranous staining with a variable component of cytoplasmic staining. The percentage of tumor cells positively stained for PDL1 was determined by pathologists. Because there are no established criteria for high PDL1 expression in lymphoma, we used the cutoff value of 50% which was suggested by the manufacturer’s instructions of PDL1 IHC 22C3 pharmDx kit [8]. Thus, PDL1 expression was defined as follows: No expression (PDL1-positive tumor cells < 1%), low expression (PDL1-positive tumor cells 1%-49%), and high expression (PDL1-positive tumor cells ≥ 50%).
4. Study parameters
The response of each patient was classified based on the best response during pembrolizumab treatment, regardless of the final outcome. The overall response rate (ORR) was based on the number of patients who achieved a complete response (CR) or a partial response (PR). The toxicity profiles of pembrolizumab were determined based on review of the medical records. The number of previous treatments was defined as the total number of cycles of treatment from the first-line chemotherapy to the last chemotherapy before pembrolizumab. Radiotherapy or autologous or allogeneic stem cell transplantation (SCT) were not included in the number of previous treatments because they were used as adjuvant or consolidation therapy. The characteristics of patients including age, performance status, stage, and absolute lymphocyte count were recorded at the time of pembrolizumab treatment, not at the time of diagnosis. Time to pembrolizumab was defined as the interval between the date of diagnosis and the date of the first infusion of pembrolizumab. Post-pembrolizumab survival was defined as the time between the date of first infusion of pembrolizumab and the date of last follow-up or death from any cause. The participants’ disease status and survival were updated on December 31, 2017.
Results
1. Characteristics of patients before pembrolizumab
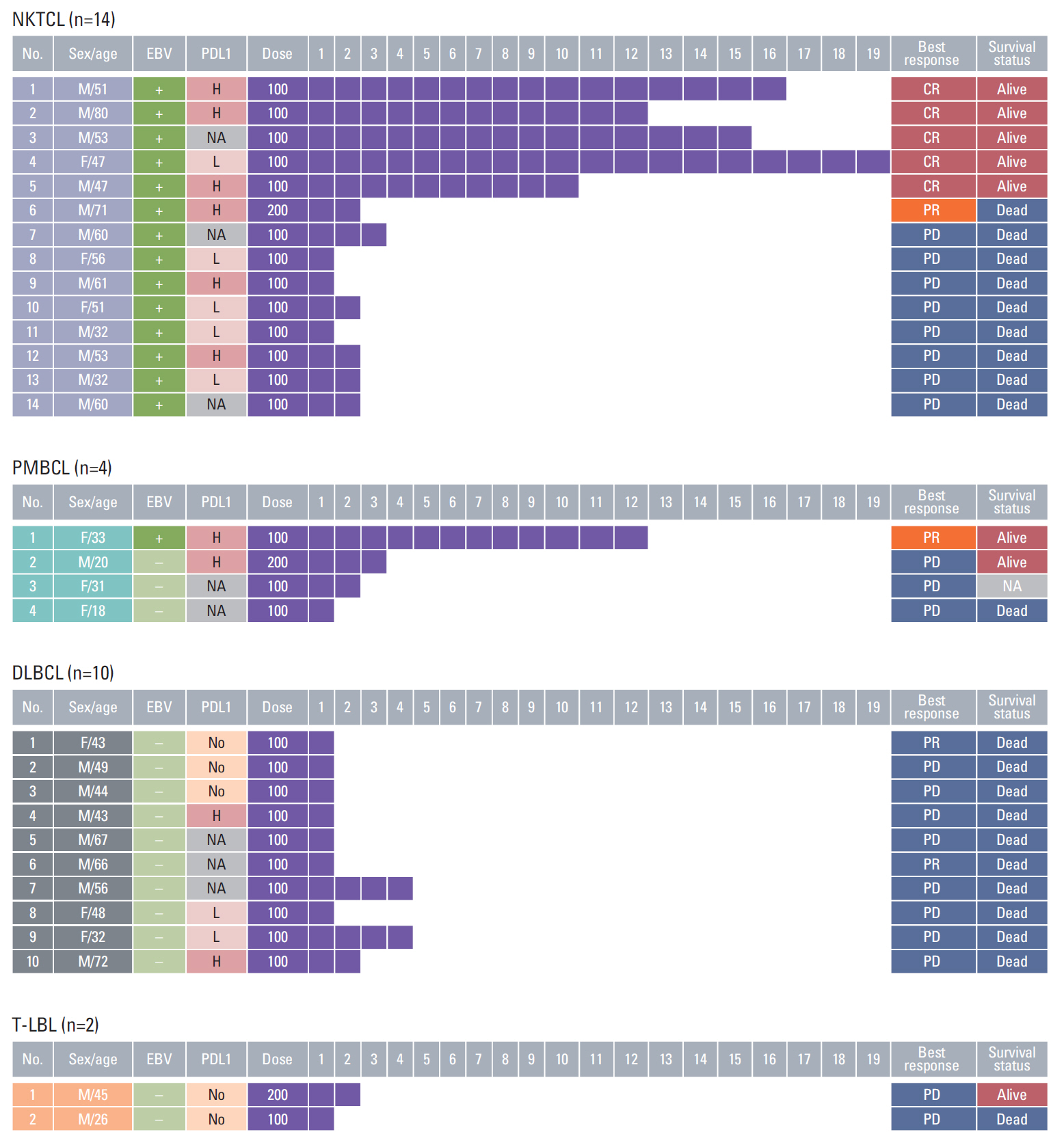
The median age of patients at the time of pembrolizumab treatment was 49 years (range, 18 to 80 years) and most were men (n=27). The histologic subtypes of tumor were diffuse large B-cell lymphoma (DLBCL; n=10), primary mediastinal large B-cell lymphoma (PMBCL; n=4), NKTCL (n=14), and T-cell lymphoblastic lymphoma (T-LBL; n=2). Most patients had stage IV disease (n=26) with widespread organ involvement (≥ 2 sites of extranodal involvement, n=25) (Table 1). The majority of patients had been heavily treated before pembrolizumab treatment: the median number of previous chemotherapy treatments excluding SCT was 4 (range, 1 to 10), and 16 patients had undergone autologous or allogeneic SCT (Table 1). Five patients had relapsed after allogeneic SCT, including one patient who underwent haploidentical SCT. All patients with DLBCL and T-LBL showed negativity for EBV whereas all cases of NKTCL and one case of PMBCL were positive for EBV (Table 1).
2. Response to pembrolizumab
All patients with DLBCL rapidly progressed during pembrolizumab treatment and died. Therefore, more than half the patients discontinued pembrolizumab after their first cycle (median number of cycle, 1; range, 1 to 4). The two patients with T-LBL had relapsed after haploidentical and unrelated allogeneic SCT and received pembrolizumab as a salvage treatment. However, their disease rapidly progressed after the first of second cycle of pembrolizumab. Of the four patients with PMBCL, case 1 showed a PR, and completed the 12th cycles of pembrolizumab (Fig. 1). She is currently in the state of ongoing treatment. On the contrary to other tumor subtypes, six NKTCL patients responded (5 CR, 1 PR; ORR, 44%). Case 1 who had relapsed after unrelated allogeneic SCT, showed a CR: this case was included in a previous study [5]. Since then, he has continued to receive pembrolizumab up to 16 cycles, and has shown no clinical or radiologic evidence of disease relapse during treatment (Fig. 1). Case 2, an 80-year-old man who was diagnosed with stage IV NKTCL only received a half-dose of SMILE (steroid, methotrexate, ifosfamide, L-asparaginase, and etoposide) chemotherapy because he was elderly and unsuitable for intensified chemotherapy. After his third cycle of SMILE chemotherapy, his disease progressed with an elevation in blood EBV DNA titer (90,568 copies/mL). However, he achieved CR with an undetectable level of blood EBV DNA after the third cycle of pembrolizumab and completed 12 cycles. Three patients (case 3-5) also continued to receive pembrolizumab up to 19th cycle (Fig. 1). Case 6 showed a PR after the second cycle of pembrolizumab, but the patient refused further treatment for financial reasons; his disease progressed, and he died (Fig. 1). Most patients who showed disease progression after one to three cycles of pembrolizumab died.
3. Adverse events during pembrolizumab treatment
Case 1 with NKTCL developed a grade II skin rash after the third cycle of pembrolizumab treatment. The biopsy of skin lesion showed hydropic degeneration and basal vacuolization consistent with graft-versus-host disease (GVHD). Although the time to onset of skin lesion was longer than 1 year because he underwent allogeneic SCT from a matched unrelated donor 10.6 months before pembrolizumab treatment, we reported this event as an acute GVHD in a previous study [5]. The reason was that he did not have any sign of acute GVHD before pembrolizumab and his skin manifestation was not consistent with chronic GVHD. His skin lesions improved with corticosteroid treatment and further therapy was unhindered. In contrast, cases 1 and 2 with T-LBL did not develop any sign of GVHD despite having undergone haploidentical and unrelated allogeneic SCT 11.0 and 6.2 months before pembrolizumab treatment. Case 9 with NKTCL involving the small intestine developed bowel perforation after the first cycle of pembrolizumab and died as a result of sepsis (Fig. 1).
4. Association of PDL1 with EBV positivity
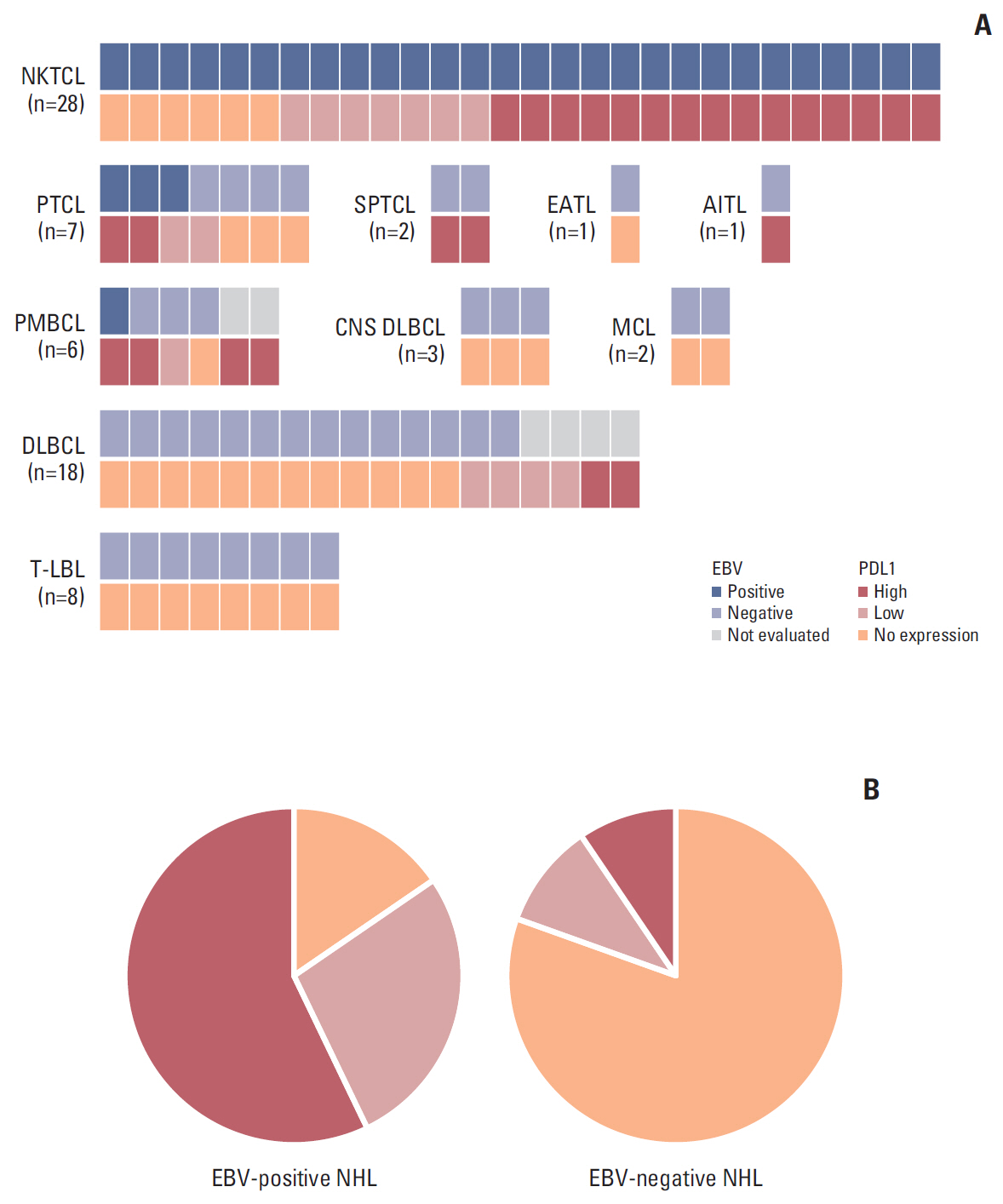
PDL1 expression was evaluated in archived tumor tissue samples from 76 patients with NHL including 21 patients treated with pembrolizumab. The proportion of tumors with high PDL1 expression differed according to the subtype of NHL. Thus, high PDL1 expression was more frequent in NKTCL (15/28, 54%), PMBCL (4/6, 67%), and peripheral T-cell lymphoma (PTCL; 2/7, 29%) than in DLBCL (2/18, 11%) and T-LBL (0/8, 0%). Although the numbers were small, high PDL1 expression was observed in subcutaneous panniculitis-like T-cell lymphoma and angioimmunoblastic T-cell lymphoma unlike primary central nervous system (CNS) DLBCL (0/3), mantle cell lymphoma (0/2), and enteropathy-associated T-cell lymphoma (0/1) (Fig. 2A). Although six patients were not evaluated for EBV in situ hybridization including DLBCL (n=4) and PMBCL (n=2), EBV-positivity was more frequent in NKTCL (28/28, 100%) and PTCL (3/7, 43%) than other subtypes. EBV-positive NHL included a significantly higher proportion of tumors with high PDL1 expression (18/32, 56%) compared with EBV-negative NHL (4/38, 11%, p < 0.001) (Fig. 2B). Thus, these results suggest the association of EBV-positivity with PDL1 expression although EBV-positivity was not evaluated in four cases of high PDL1 expression due to lack of available tissue (DLBCL and PMBCL) (Fig. 2A).
5. Association of PDL1 and EBV positivity with treatment outcome
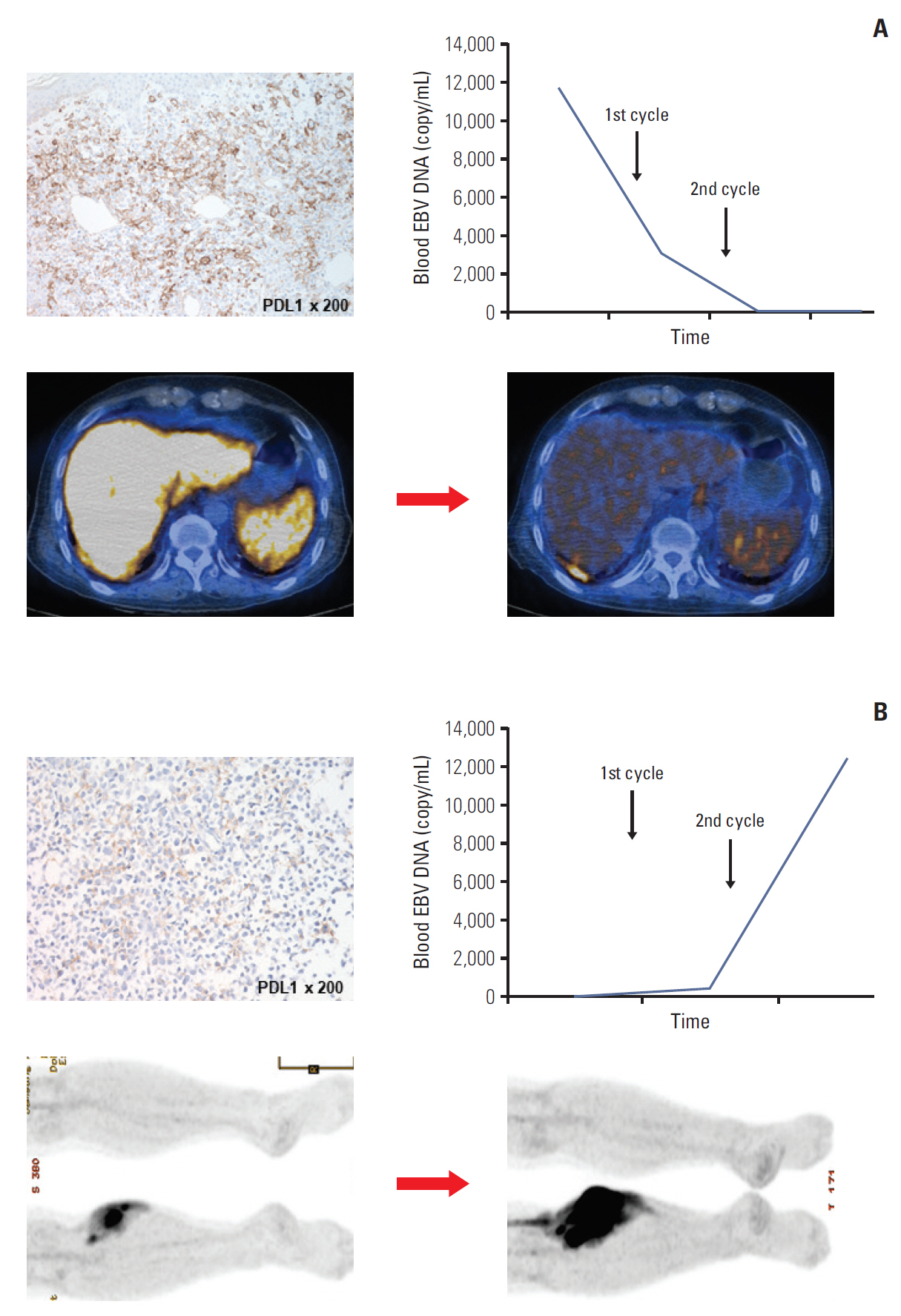
When we dichotomized 30 patients receiving pembrolizumab into two groups according to the EBV positivity, seven patients with EBV-positive tumor responded to pembrolizumab (7/15) whereas all patients with EBV-negative tumor failed to respond (0/15) (Table 2). Thus, NKTCL (6/14, 44%) and PMBCL (1/4, 25%) showed higher ORR than DLBCL (0/10, 0%) and T-LBL (0/2, 0%). This higher response to pembrolizumab was associated with more frequent expression of PDL1 in EBV-positive tumors. Indeed, aforementioned case 1 of PMBCL who had EBV-positive disease and high PDL1 expression showed a PR to pembrolizumab (Fig. 1). The different proportions of high PDL1 expression in different subtypes of NHL tumors correlated with their response to pembrolizumab. Of 21 pembrolizumab-treated patients whose PDL1 expression was analyzed, five cases with high PDL1 expression responded to pembrolizumab (5/10, 50%) whereas only two cases with low PDL1 expression responded (2/11, 18%); however, this difference was not significant (p=0.183). Even in patients with NKTCL, the ORR was different between those with high (4/6, 67%) and low PDL1 expression (1/5, 20%). For example, case 6 of NKTCL with high PDL1 expression showed a PR with undetectable levels of EBV DNA in blood after pembrolizumab treatment (Fig. 3A), whereas case 10 with low PDL1 expression did not respond (Fig. 3B). However, this difference of response based on PDL1 expression could not be statistically analyzed due to small number of patients.
Discussion
In our study, pembrolizumab was used in different NHL subtypes, and their response to pembrolizumab was different. Thus, the ORR of NKTCL (6/14, 44%) was higher than that of PMBCL (1/4, 25%), DLBCL (0/10, 0%), or T-LBL (0/2, 0%). Although the number of patients in each subtype was small, our findings are consistent with those of a previous case series reporting outstanding outcomes of pembrolizumab treatment in NKTCL patients (Table 3). Actually, pembrolizumab as an off-label treatment for relapsed or refractory T- or NK-cell NHL achieved CR [5,9,10]. Of the patients with PMBCL, case 1 who was EBV positive with high PDL1 expression responded to pembrolizumab (Fig. 1). However, the other three patients with PMBCL, including one patient with high PDL1 expression, failed to respond. In a previous phase 1b study, the ORR to pembrolizumab was 41% (7/17) in relapsed or refractory PMBCL [11]. Although our response rate in PMBCL was inferior to these phase 1b results, the number of patients in our study was too small to draw definite conclusions about the efficacy of pembrolizumab in PMBCL. On the other hand, a recent phase II study using pembrolizumab plus rituximab reported 80% of ORR in relapsed or refractory follicular lymphoma [12]. This suggests the role of pembrolizumab as a combination treatment with other drugs. Indeed, a patient with double-hit lymphoma receiving pembrolizumab and lenalidomide achieved CR [13]. In our study, although not all patients responded to pembrolizumab, six cases of NKTCL did respond. Therefore, given that NKTCL usually follows an aggressive clinical course after relapse and there is currently no effective salvage treatment for NKTCL, our findings suggested that pembrolizumab could be a useful treatment option for relapsed or refractory NKTCL.
This different response of different NHL subtypes to pembrolizumab could be related to their different levels of PDL1 expression. Thus, our study analyzed the extent of PDL1 expression in 76 patients with NHL including 21 patients who received pembrolizumab. The frequency of high PDL1 expression was very rare in patients with DLBCL (2/18, 11%) and mantle cell lymphoma (0/2, 0%) in our study. Previous studies also reported the absence of PDL1 expression in mantle cell lymphoma [14,15]. Although those studies showed higher frequency of PDL1 expression in DLBCL than that of our study, it might be related with low cutoff value (5%) for PDL1 expression (Table 4). Actually, a study analyzing 1,253 patients with DLBCL showed the same incidence of PDL1 expression (132/1,253, 11%) as ours and the study used 30% of cutoff value [16]. Thus, the poor response to pembrolizumab in DLBCL patients of our study could be explained the low frequency of PDL1 expression. The main mechanism of PDL1 overexpression was amplification of chromosome 9p24.1, and is commonly observed in patients with HL [17]. However, the rearrangement of 9p24.1 leading to PDL1 overexpression was more frequently found in PMBCL and primary CNS DLBCL [18,19]. Our study also showed frequent PDL1 expression in PMBCL comparable to that of previous studies [14,15]. However, three cases of primary CNS DLBCL showed no expression of PDL1 unlike a previous study reporting 38% in Western patients [20]. This might be related with ethnic difference as well as a different cutoff value (50% vs. 1%). Thus, it should be evaluated in the future study using a larger study population. Our study showed high PDL1 expression in more than 50% of patients with NKTCL, and previous studies also reported high frequency of PDL1 expression [21,22]. This could be related with that tumor cells of NKTCL are invariably infected with EBV because EBV infection of tumor cells and activation of the inflammation-related JAK/STAT pathway also could upregulate PDL1 expression [24]. Other subtypes of NHL also had EBV-positive tumor cells although its frequency was lower than NKTCL. The frequency of EBV-positivity was known as approximately 10% in DLBCL, thus, some cases of EBV-positive DLBCL might have PDL1 expression [16]. However, considering poor response to pembrolizumab in DLBCL patients, even in case of high PDL1 expression, pembrolizumab should be very cautiously used in DLBCL patients (Fig. 1). Thus, it should be determined whether PDL1 is expressed on lymphoma cells before pembrolizumab treatment is initiated. Although only two patients with T-LBL received pembrolizumab, it cannot be recommended for this disease entity because PDL1 expression is absent in T-LBL. Overall, these results suggest that PDL1 expression on lymphoma cells might be useful as a biomarker predicting the response to pembrolizumab.
However, our study has several limitations as follows. First, we defined high PDL1 expression based on the cutoff value of 50% because there are no established criteria for high PDL1 expression in lymphoma. Thus, the frequency of high PDL1 expression in lymphoma patients might become different according to the cutoff values. However, a previous study for the development of a companion diagnostic PDL1 IHC assay for pembrolizumab therapy in non-small-cell lung cancer (NSCLC) showed the treatment effect of pembrolizumab was substantial in patients with ≥ 50% of PDL1-postitive tumor cells [25]. Furthermore, a phase III trial with pembrolizumab for NSCLC also reported a significant association of longer survival outcome with PDL1 expression on at least 50% of tumor cells [26]. Therefore, our cutoff value could be used to define high PDL1 expression in lymphoma although further studies with a larger study population should be performed to determine the correlation of response to pembrolizumab with PDL1 expression in lymphoma patients. Second, we used two types of antibodies to assess PDL1 expression. This might influence the results of PDL1 expression in our study. However, our pathology confirmed no difference of efficacy in analyzing the PDL1 expression between two types of assay. Furthermore, given the range of low and high PDL1 expression was wide (1%-49% vs. ≥ 50%), the use of two types of IHC assay might not complicate interpretation of IHC results. Third, most tissues samples for PDL1 expression were obtained from the time of diagnosis. Considering PDL1 expression might be different between diagnosis and relapse/progression, some patients showing the discrepancy of response and PDL1 expression might be associated with this limitation. Fourth, a substantial number of patients discontinued to receive pembrolizumab due to disease progression in our study (Fig. 1). Although it could be interpreted as a lack of efficacy in those patients, the probability of atypical response patterns mimicking disease progression could exist because immune-reaction inducing tumor-flare or pseudoprogression could be found in the treatment with pembrolizumab in other solid tumors. Thus, response evaluation and the assessment of disease status should be more careful in lymphoma patients receiving pembrolizumab as the refinement of the Lugano Classification Response Criteria for Lymphoma was proposed in the era of therapy with immune checkpoint inhibitor [27]. Fifth, the number of each subtype was small, especially T-LBL, and there is lack of data about the outcome of other subtypes such as mantle cell lymphoma. Thus, future study with a larger study population including more subtypes should be warranted. Lastly, the dosage of pembrolizumab given to most patients (100 mg every 3 weeks) was lower than that recommended (200 mg every 3 weeks). However, in our study the efficacy of treatment with pembrolizumab was comparable with those reported in previous studies (Table 2), and was consistent with the results of a study suggesting that low-dose pembrolizumab (100 mg every 3 weeks) could be effective for relapsed or refractory HL, with minimal toxicity [28]. In fact, when using this low dose of pembrolizumab we observed six responders (2 CR, 4 PR) out of eight patients with relapsed or refractory HL who failed treatment with brentuximab vedotin and autologous SCT (ORR, 75%) (S1 Table). The outcome of our low-dose treatment was comparable to that of previous phase II studies of relapsed or refractory HL that reported an ORR of 65% (16% CR) using 10 mg/kg of pembrolizumab every 2 weeks [29] and an ORR of 69% (22.4% CR) using 200 mg of pembrolizumab every 3 weeks [30].
None of the patients in our study showed any grade 3 or 4 hematologic or nonhematologic toxicities, and their causes of death were related to disease progression. Although one patient developed a bowel perforation, that patient had previously experienced bowel perforation during salvage chemotherapy before initiation of pembrolizumab treatment. Therefore, the toxicity of pembrolizumab was manageable, which might be because we used a low dose of 100 mg of pembrolizumab every 3 weeks, although a previous study using 10 mg/kg of pembrolizumab every 2 weeks reported five cases of grade 3 drug-related adverse events (16%). Furthermore, five patients in our study had undergone unrelated or haploidentical allogeneic SCT before receiving pembrolizumab, but only one patient developed grade II acute GVHD (case 1 with NKTCL) (Fig. 1). This might be related to the lower dose of pembrolizumab and be consistent with the safety of PD1 blockade after allogeneic SCT [10].
In conclusion, pembrolizumab could be useful as a salvage treatment for relapsed or refractory EBV-positive NHL, especially NKTCL. However, its efficacy in EBV-negative NHL with low or absent PDL1 expression is still not clear although pembrolizumab could be a potential treatment option for relapsed or refractory NHL.