INTRODUCTION
Pancreatic cancer is the cause of 5.7 per 100,000 estimated deaths in Korea, and it was the fifth leading cause of cancer deaths in the year 2002 (1).
The only curative treatment option for pancreatic cancer is complete surgical resection, but only 5% to 25% of these patients who present with pancreatic cancer are candidates for resection. At the time of diagnosis, most patients have locally advanced and/or metastatic disease and they experience severe pain, nausea and emesis, anorexia and significant weight loss. Those symptoms have a substantial negative effect on the patients' performance status (PS) and quality of life. The median survival for these patients ranges from 3 months to 6 months (2).
Chemotherapy is widely used for the treatment of patients with advanced stage pancreatic cancer in an attempt to improve survival and to control the disease-related symptoms (3,4). Gemcitabine is currently the most active agent to treat locally advanced or metastatic pancreatic cancer (2,5). Many attempts have been made to increase the overall objective response rate and the survival of patients with locally advanced or metastatic pancreatic cancer, and particularly by combining gemcitabine with other drugs. It has been shown that cisplatin has a 21% overall objective response rate with a median overall survival (OS) of only 4 months for patients with locally advanced or metastatic pancreatic cancer (6).
Although the activity of cisplatin alone may be overestimated, it has been shown that the gemcitabine-cisplatin combination is synergistic in vitro because gemcitabine is able to inhibit DNA repair after cisplatin-induced damage, and cisplatin is able to influence gemcitabine catabolism through the inhibition of ribonucleotide reductase (7,8). Yet the effectiveness of combining cisplatin with gemcitabine is still controversial (9,10).
Therefore, we performed a retrospective analysis of the treatment outcomes of gemcitabine versus gemcitabine combined with cisplatin for patients with locally advanced or metastatic pancreatic cancer.
MATERIALS AND METHODS
1) Patients
From 2001 to 2007, we enrolled 60 patients who were administered gemcitabine or gemcitabine combined with cisplatin as treatment for locally advanced or metastatic pancreatic cancers. They met the following inclusion criteria; 1) they had an imaging diagnosis of locally advanced and/or metastatic pancreatic carcinoma; 2) they had measurable disease, as defined by the Response Evaluation Criteria in Solid Tumors (RECIST) (11); 3) they were 18 years or older in age 4) they had an adequate baseline bone marrow reserve (white blood cell count ≥4,000/mm3, hemoglobin level ≥10 g/dl, platelets ≥100,000/mm3), adequate hepatic function (a level of transaminases ≤2.5 times the normal values) and adequate renal function (defined as a serum creatinine concentration ≤1.5 mg/dl and a blood urea nitrogen level ≤50 mg/dl) and 5) they had a Eastern Cooperative Oncology Group (ECOG) PS of 0, 1 or 2.
2) Treatment schedule
Gemcitabine (G) was diluted in normal saline and it was administrated at 1,000 mg/m2 on day 1 and day 8 every 3 weeks. Cisplatin was added at 60 mg/m2 on day 1 every 3 weeks to the gemcitabine schedule (GP). The WHO toxicity criteria were used in this study and we recorded the incidence of grade III~IV toxicity.
3) Pretreatment and follow-up studies
Imaging studies were done by performing abdominal computed tomography scans (CT), and this documented the patients' measurable disease before treatment. Obtaining the medical history, physical examinations, complete blood cell counts, a serum chemistry panel and chest X-rays were carried out before each cycle of therapy. Abdominal CT was carried out each 3 cycles of chemotherapy.
4) Response evaluation
The responses to chemotherapy were graded according to the RECIST criteria (11). A complete response (CR) was defined as disappearance of all measurable lesions, no new lesions and normalization of the tumor markers for at least 4 weeks. A partial response (PR) was defined as a 30% decrease in the sum of the longest diameter of the measurable lesions from baseline, non-progressive disease in the non-targeted lesions and no lesions. Progressive disease (PD) was defined as a 20% increase in the sum of the longest diameter of the measurable lesions or the appearance of new lesions. Stable disease (SD) was defined as small changes that do not meet the above criteria. The dose intensity (mg/m2/week) was calculated as the total cumulative dose divided by the duration of treatment. The relative dose-intensity (RDI) was calculated by dividing the dose-intensity by the planned dose-intensity, and this was expressed as a percentage. The planned dose-intensities, expressed as mg/m2/week, were 667 for gemcitabine and 20 for cisplatin.
5) Statistical methods
All analyses were performed with the use of SPSS software (version 12.0, Chicago-IL). The differences in the clinical characteristics between the two groups for the OR rates were analyzed by a chi-square test. Statistical analysis was performed by the log-rank test to compare differences in progression free survival (PFS) and OS between the two groups. Survival curves were constructed by using the Kaplan-Meier method.
RESULTS
1) Patient characteristics and the disease status
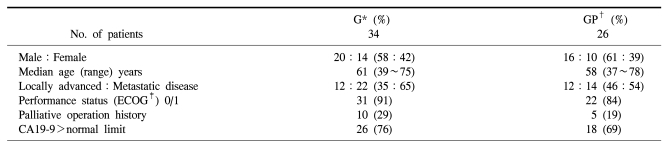
Sixty patients were enrolled in this study. The patients' characteristics and disease status are listed in Table 1. Thirty four patients received gemcitabine (G) and 26 patients received gemcitabine combined with cisplatin (GP). The locally advanced disease and metastatic disease percentages were 35% and 65% in group G, and 46% and 54% in group GP. Twenty patients were male (58%), and 14 patients were female (42%) in group G, and 16 patients were male (61%) and 10 patients were female (39%) in group GP. Ten patients in group G (29%) and 5 patients in group GP (19%) had undergone a previous palliative operation. Twenty six patients in group G (76%) and 18 patients in group GP (69%) showed a recorded rise of their CA 19-9 level.
2) Treatment, the response and survival
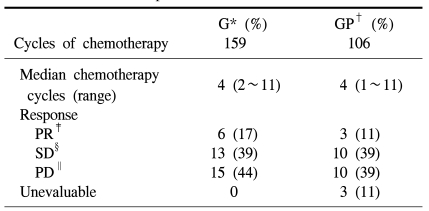
The median follow-up duration was 29 months (range: 7~64 months). The response rates are showed in Table 2. The median number of administered cycles in group G and group GP was 4 (range: 1~11 cycles) and 4 (range: 2~11 cycles), respectively. The PR rate of group G was 17% and that of group GP was 11%. The SD rate was 39% in both groups. The PD rate of group G was 44% and that of group GP was 39% (p=0.719). The total number of chemotherapy cycles for group G was 159 and that of group GP was 106 (p=0.410).
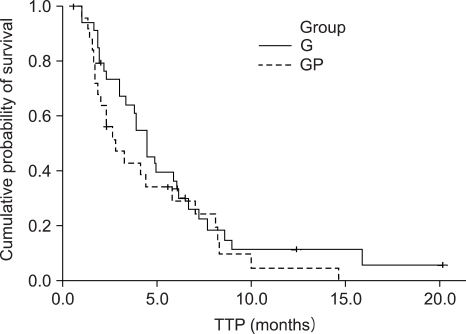
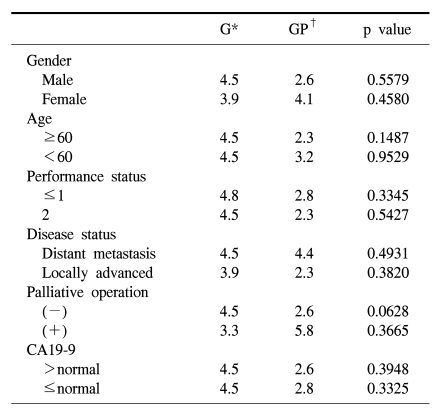
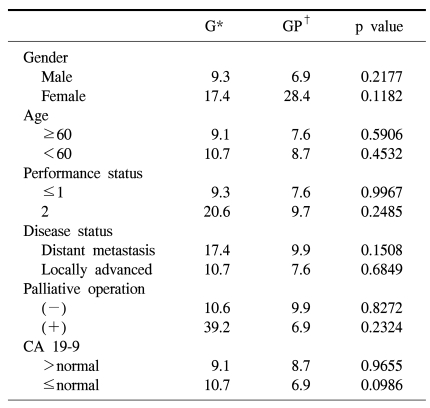
The median PFS was 4.5 months (95% CI: 3.6~5.4) for group G and 2.8 months (95% CI: 1.4~4.2) for group GP. The median OS was 10.7 months (95% CI: 1.1~20.3) for group G and 8.7 months (95% CI: 5.0~12.4) for group GP. Yet there was statistical difference in the PFS (p=0.2396) (Fig. 1) and OS (p=0.4643) between the 2 groups (Fig. 2).
3) Toxicities
Sixty patients received a total of 265 treatment cycles. Thirty four patients received a total of 159 cycles with gemcitabine treatment and 26 patients received a total of 106 cycles with gemcitabine combined with cisplatin treatment. The median cumulative doses were 940 mg/m2 gemcitabine (range: 750~11,000) in group G, and 966 mg/m2 gemcitabine (range: 750~9,000)- 57 mg/m2 cisplatin (range: 45~540) in group GP. Dose reductions were required 8 times each in both groups. The dose intensity for group G was 626 gemcitabine mg/m2/week and that for group GP was 644 mg/m2 gemcitabine/week- 19 mg/m2 cisplatin/week, and the RDI of group G was 94.8% and that for group GP was gemcitabine 97.5%- cisplatin 95%.
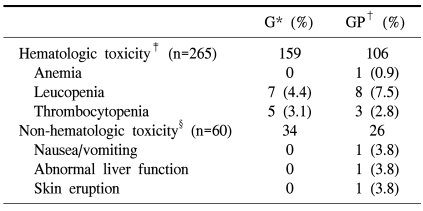
The toxicities observed during the treatment are listed in Table 3. The hematological toxicity profile was similar in both groups: grade III-IV neutropenia and thrombocytopenia was observed in 4.4% and 3.1%, respectively, of the patients in group G and in 7.5% and 2.8%, respectively of the patients in group GP. But non-hematological toxicities (skin rash, abnormal liver function test, nausea/vomiting) were observed in 3 patients of group GP.
DISCUSSION
Gemcitabine is currently considered by most oncologists as the standard treatment for patients with advanced pancreatic carcinoma, and this is based on the results obtained in phase II-III trials, These trials reported a clinical, beneficial response in 23~40% of the patients, a major OR rate ranging from 5.4% to 16.6%, disease stabilization in 19~40% of the patients, and a median OS ranging from 3.9 months to 6.3 months (12).
To improve the clinical results of gemcitabine for treating advanced pancreatic carcinoma, some recent phase II-III trials have evaluated the efficacy of combinations of gemcitabine with other drugs such as 5-FU, cisplatin, topoisomerase I inhibitors etc., and these drugs have been shown to be synergistic in vitro (13). Some trials demonstrated that gemcitabine-based combination chemotherapy improved the response rate, the PFS and the median OS compared with gemcitabine alone. On comparing gemcitabine plus erlotinib with gemcitabine plus placebo, the one-year survival and progression-free survival were significantly longer for the patients who were administered erlotinib plus gemcitabine (14). In patients with a good PS, gemcitabine-doublelets may be the new standard treatment. On comparing gemcitabine with gemcitabine plus capecitabine, the patients with good a KPS (score of 90 to 100) showed a significant prolongation of their median OS duration in the gemcitabine plus capecitabine group compared with the patients in the gemcitabine group (15). Yet there have not been enough phase III studies, so a single agent is now considered as the standard treatment for patients with advanced pancreatic cancer.
In our study, gemcitabine single treatment was more tolerable and it had the same efficacy as compared with gemcitabine and cisplatin combination treatment: there were no significant differences in the PFS and OS. None of the predictive factors favored combination therapy. The hematological toxicity profile was similar for both groups, but the non-hematological toxicities were higher for the GP group for nausea/vomiting, abnormal LFT and skin eruption. The results presented here show that the GP group seems to experience more toxicity than the G group.
CONCLUSION
The gemcitabine plus cisplatin combination had no significant survival benefit and had toxicities that of gemcitabine alone in patients with locally advanced or metastatic pancreatic cancer. Our study had limitations as a retrospective analysis of treatment, the stratification of both groups, the small sample size (the required number of patients was >500), and the short duration of the survival gain (2 wks~2 mos). Therefore, well designed prospective, large scale studies that will focus on gemcitabine versus gemcitabine combination treatment are needed in the future.