Depression, Rather Than Cancer-Related Fatigue or Insomnia, Decreased the Quality of Life of Cancer Patients
Article information
Abstract
Purpose
Cancer-related fatigue is a common and distressing symptom that occurs during cancer treatment. This study aimed to find factors that are related to cancer-related fatigue, and its effect on patients’ quality of life.
Materials and Methods
This study included 159 patients who completed questionnaires and interviews during their initial examination at the sleep clinic for cancer patients, Asan Medical Center, between December 2018 and January 2020. Their medical reports were reviewed retrospectively. Questionnaire data about depression, anxiety, insomnia, fear of disease progression, and dysfunctional beliefs about sleep, pain, and quality of life, were reviewed. Additionally, patient sleep structure data were analyzed.
Results
Factors such as depression (p < 0.001), anxiety (p < 0.001), fear of cancer progression (p < 0.001), fatigue (p=0.027), and time in bed during 24 hours (p=0.037) were significant expecting variables for low quality of life from logistic regression analysis. In pathway analysis, depression (p < 0.001), not cancer-related fatigue (p=0.537), act as a direct risk factor on quality of life. And also, depression was an overall risk factor for insomnia, fatigue, and daily activity of cancer patients.
Conclusion
Cancer-related fatigue did not show significant effect on patient’s quality of life in this study. However, the result of pathway analysis highlights the importance of assessing depression in the process of cancer treatment and providing appropriate interventions.
Introduction
Cancer-related fatigue is a common and painful side effect that occurs over the course of cancer treatment [1]. The clinical guidelines of the National Comprehensive Cancer Network defines cancer-related fatigue as a distressing, persistent, subjective sense of physical, emotional, and/or cognitive tiredness or exhaustion related to cancer or cancer treatment that is not proportional to recent activity and interferes with usual functioning [2]. Numerous studies report that approximately 30%–60% of cancer patients experience moderate or worse levels of cancer-related fatigue symptoms, leading some patients to stop their cancer treatment [3]. Cancer-related fatigue can occur before the commencement of cancer treatments and it tends to increase during the process of radiotherapy or chemotherapy [4,5].
Cancer-related fatigue typically improves within a year after the completion of cancer treatments; however, 25%–30% of patients continue to experience these symptoms for several years after the successful completion of cancer treatments [6,7]. Cancer-related fatigue manifests through diversified physical, psychological, and emotional clinical symptoms, affecting the overall quality of life of cancer patients [7,8].
Cancer-related fatigue can be affected by diverse demographic, medical, psychosocial, behavioral, and biological factors [9]. The underlying mechanisms of cancer-related fatigue are associated with abnormal cytokine control, hormonal secretion of hypothalamus-pituitary gland-adrenal gland axis, and 5-hydroxytryptophan neurotransmitter control [10]. The precise physiological mechanism that induces cancer-related fatigue is not fully understood; however, psychological factors, such as depression and anxiety, and sociocultural factors, such as biorhythm, act together with these physiological factors [11].
The aim of this study is to explore whether the cancer-related fatigue may be the most important factor for the quality of life of cancer patients. We sought to examine cancer-related fatigue by confirming its correlation with clinical indices, including depression, anxiety, insomnia, quality of life, dysfunctional belief on sleep, and sleep structure. Moreover, we sought to examine the pathway by which cancer-related fatigue interacts with these clinical indices to affect the quality of life of patients with cancer.
Materials and Methods
1. Patients
This study was conducted on all patients capable of completing a questionnaire and interview at their initial examination among the patients who visit the sleep clinic for cancer patients of Asan Medical Center between December 1, 2018, and January 31, 2020. Patients who could not complete the questionnaire or be interviewed due to any communication disability were excluded from the study. Patients with accompanied mental disorders, such as delusion or psychosis, were also excluded.
2. Study design
The questionnaire included the Insomnia Severity Index (ISI), Patient’s Health Questionnaire-9 (PHQ-9), Fear of Progression (FoP), State subcategory of State and Trait Anxiety Inventory (STAI), Cancer related Dysfunctional Beliefs about Sleep (C-DBS), WHO-5 questionnaire, Pain Numeric Rating Scale (Pain NRS), and Fatigue Numeric Rating Scale (Fatigue NRS), which patients were required to complete at their initial examination.
The results were assessed by reviewing the medical records of the patients who visited the Cancer Stress and Sleep Clinic of Asan Medical Center between December 1, 2018 and January 31, 2020. Sleep structure was assessed using time to bed, sleep onset, and wake; sleep onset latency (SL); total time in bed (TIB); total time in bed during 24 hours (TIB/d); and total time in bed during the daytime (TIB/daytime). In addition, demographic data, including the sex, age, type and stage of cancer diagnosis, current status of treatment (anti-cancer treatments, radiotherapy, immunotherapy, and/or hormonal therapy), medical history of surgery over the last 3 months, and other medications, was analyzed.
Mutual correlations among the clinical indices, including depression, anxiety, insomnia, dysfunctional thinking on sleep, and fear of cancer progression; sleep-related indices; cancer-related fatigue; and quality of life were analyzed to examine the risk factors that affect the quality of life and fatigue symptoms of cancer patients.
3. Assessment tools
The PHQ-9 was used to assess depression symptoms [12]. This is a self-report type questionnaire of nine questions, including unpleasantness, depression, insomnia, fatigue, loss of appetite, feeling of guilt, degradation of concentration, delay in mental exercises, and thoughts on suicide/self-infliction. The STAI was used to assess anxiety [13]. This is a self-report type questionnaire composed with a 4-point Likert scale that includes questions on the state and traits of anxiety. In this study, items of the subordinate category for the state of anxiety were used. The ISI was used to assess insomnia-related anxiety [14]. This includes seven self-report type questions on insomnia symptoms. Each question is measured using a 0–4 point Likert scale; higher scores indicate more severe insomnia symptoms. The C-DBS was used to assess dysfunctional thinking about sleep in cancer patients [15]. This is composed of two questions: “My immune system will have serious problems if I don’t go to sleep at a certain time” (Q1-immune) and “If I don’t sleep well at night, my cancer may recur or metastasize” (Q2-recurrence). Patients are instructed to score their responses from 0–10 for each question. The sum of the scores is calculated as the C-DBS score. The FoP questionnaire was used to assess the extent of fear towards the aggravation of patients with chronic diseases [16]. This is composed of 43 questions that are grouped into subcategories relating to ‘anxiety’ and ‘adaption.’ Each question is measured with score in the range of 1–5 points. The Korean translated version of the FoP Questionnaire Short Form (FoP-Q-SF), which is composed of 12 questions, was used [17,18].
The WHO-5 Questionnaire was used to assess the quality of life of patients [19]. This is composed of five questions that are scored in the range of 0–5. The sum of the scores is calculated and multiplied by 4 to provide an overall quality of life score (0–100). The Fatigue NRS [20,21] and the Pain NRS [22] were used to assess cancer-related fatigue and pain, respectively.
4. Statistical analysis
Spearman’s correlation analysis was performed to assess the correlation between the self-report questionnaires (PHQ-9, ISI, STAI, FoP, and C-DBS). Additional correlation analyses were performed to measure the association between sleep indices (SL, TIB/d, TIB/daytime) the self-report questionnaires. Patients were divided into groups based on their Fatigue NRS scores; one group included those who reported extensive fatigue (scores of 8–10, accounting for the top 25% of patients) and one group included those without extensive fatigue (scores of 0–7, accounting for the bottom 75% of patients). Student’s t test and chi-square test were performed to analyze the differences questionnaire scores, sleep indices, and other clinical indices between groups.
To assess the factors associated with differences in quality of life, patients were divided into groups based on their WHO-5 Questionnaire scores; one group included those who reported low quality of life (scores of 0–12, accounting for the bottom 25% of patients) and one group included those who reported high quality of life (scores of 16–80, accounting for the top 75% of patients). Student’s t test and chi-square test were performed to analyze the differences questionnaire scores, sleep indices, and other clinical indices between groups.
We hypothesized that TIB/daytime would be associated with cancer-related fatigue or quality of life. To confirm this hypothesis, comparative analysis (t test and chi-square test) was performed on the self-report questionnaire scores, cancer-related fatigue, and quality of life between patients with a TIB/daytime > 30, > 60, and > 120 minutes.
Logistic regression analysis was performed to assess the risk factors for cancer-related fatigue and quality of life. Odds ratio values were calculated with age, sex, cancer types, and psychiatric diagnosis as confounding factors. In addition, a hypothetic model of the underlying pathway of how cancer-related fatigue affects quality of life was established using existing studies [23], and pathway analysis was executed. SPSS ver. 21.0 (IBM Corp., Armonk, NY) and AMOS was used for statistical and pathway analysis. Data were considered significant when p < 0.05.
Results
Full patient demographics are described in Table 1. We found that 130 of 159 subjects (81.8%) were females and the mean age patients was 54.9 (standard deviation, 11.6) years. The proportion of cancer types were breast cancer (52.2%), lung cancer (8.8%), and pancreatic and biliary cancer (8.2%) in this patient cohort. Approximately one quarter of patients (25.2%) had undergone surgery during the last 3 months, and 8.2%, 28.3%, 30.2%, and 5.7% of patients were receiving radiotherapy, chemotherapy, hormonal therapy, and immunotherapy, respectively, at the time of the initial examination. Over half the patients reported insomnia (57.2%). Depression and acute stress reaction/adaption disorder were also reported in 22.6% and 7.5% patients, respectively.

Patient demographic and clinical characteristics
The correlations between sleep indices and self-report questionnaire scores are shown in Table 2. There were significant negative correlations of age with depression, anxiety, and fear of progression. There were significant correlations between depression and insomnia, anxiety, FoP, and C-DBS (all p < 0.01). In addition, C-DBS was significantly correlated with insomnia, depression, anxiety, and fear of cancer progression (p < 0.01). TIB/d was correlated with depression and anxiety (both p < 0.01), and it showed that a reduction in physical activity and delay in mental exercises are important characteristic of depression [24].
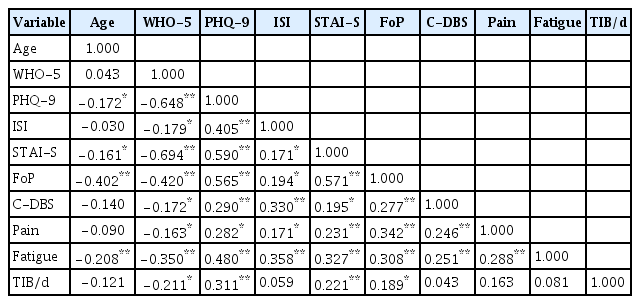
Spearman’s correlation coefficients of each variable
Comparative analysis of the questionnaire results, clinical indices, and sleep-related indices between patients with low or high quality of life are shown in Table 3. There was no significant difference in the proportion of the patients diagnosed with metastatic cancer (stage 4), or the current cancer treatment between patients with low or high quality of life. There were significant differences in depression, anxiety, and FoP scores between the low and high quality of life groups (p < 0.001). Additionally, patients reporting a lower quality of life had relatively longer TIB/daytime and TIB/d.

Comparison of self-reported questionnaire scores and sleep indices between the low and high quality of life groups
To confirm the difference in the questionnaire results and clinical indices in accordance with TIB/daytime, we compared the TIB/daytime in the low and high quality of life groups by creating subgroup analyses of patients based on their reported TIB/daytime, using 30, 60, and 120 minutes as cutoff points for each subgroup. The existing literature does not specify cutoff points for TIB/daytime; therefore, these were created based on generally recommended daytime nap times.
Logistic regression analysis (Table 4) showed that metastatic cancer diagnosis or status of cancer treatments did not significantly affect the quality of life. Among variables, only depression (p < 0.001), anxiety (p < 0.001), and fear of cancer progression (p < 0.001), fatigue (p=0.027), and TIB/d (p=0.037) were significant predicting variables for low quality of life of patients. Finally, we performed a pathway analysis using our final model hypothesis that referenced an existing pathway analysis study [23] on dysfunctional belief on sleep, fear of cancer progression, and insomnia (Fig. 1).

Risk factors related to lower quality of life (WHO-5 Questionnaire bottom 25%) group in cancer patients
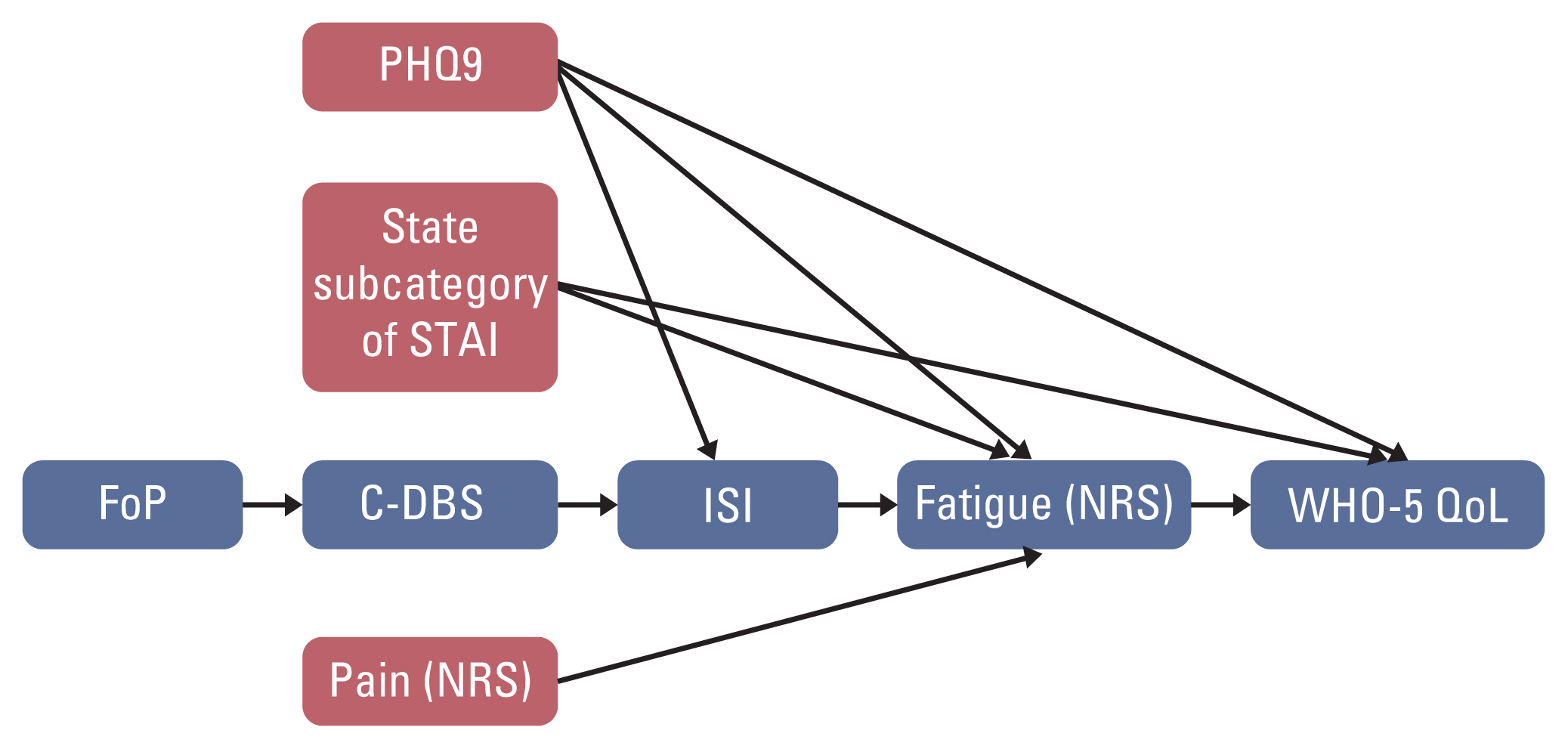
Pathway analysis hypothesis model. C-DBS, Cancer-Related Dysfunctional beliefs about Sleep; Fatigue (NRS), Fatigue Numeric Rating Scale; FoP, Fear of Progression; ISI, Insomnia Severity Index; Pain (NRS), Pain Numeric Rating Scale; PHQ-9, Patient Health Questionnaire-9; STAI, State-Trait Anxiety Inventory; WHO-5 QoL, WHO-5 Questionnaire.
The pathway analysis (Fig. 2) confirmed that depression was a risk factor for quality of life (p < 0.001), and depression also was an overall risk factor for insomnia, cancer-related fatigue, quality of life, and TIB/daytime (all, p < 0.001). Contrary to the hypothesis, cancer-related fatigue was not a risk factor for the quality of life (p=0.537). The pathway analysis also confirmed the results of the existing study that fear of cancer progression affects dysfunctional belief on sleep, which in turn aggravates insomnia [23].

Pathway analysis result. C-DBS, Cancer-Related Dysfunctional beliefs about Sleep; Faigue (NRS), Fatigue Numeric Rating Scale; FoP, Fear of Progression; ISI, Insomnia Severity Index; Pain (NRS), Pain Numeric Rating Scale; PHQ-9, Patient Health Questionnaire-9; STAI, State-Trait Anxiety Inventory; TIB/d, time in bed during 24 hours; WHO-5 QoL, WHO-5 Questionnaire.
Discussion
In this study, we observed that cancer patients’ depression, rather than cancer-related fatigue, influenced their quality of life, though we hypothesized that cancer-related fatigue symptoms, influenced by depression, anxiety, insomnia, quality of life, dysfunctional belief on sleep, and sleep structure, might be the most important factor for quality of life. In addition, patients’ fatigue, insomnia, and decreased daytime activities (increased TIB/d) were influenced by patients’ depressive symptoms, but those variables cannot have a direct impact on their quality of life.
1. Role of cancer-related fatigue among the factors that affect the patients’ quality of life
We found significant differences in self-reported scores for depression, anxiety, insomnia, dysfunctional thinking on sleep, fear of cancer progression, and pain between patients reporting low or high cancer-related fatigue. In contrast, only self-reported scores of depression, anxiety, and fear of cancer progression were significantly different between high and low quality of life groups. This was also shown in the logistic regression analysis.
Moreover, we found a significant correlation between cancer-related fatigue and quality of life in this study. This suggests that cancer-related fatigue may have an indirect mediating effect in the processing of pain, insomnia, and dysfunctional belief on sleep, which effects quality of life. Our pathway analysis confirmed that insomnia and depression symptoms act as risk factors for fatigue symptoms. In addition, the effects of fear of cancer progression and dysfunctional thinking on sleep on insomnia are consistent with the results of previous studies [23]. Although fatigue symptoms were correlated with quality of life, our analysis revealed that they did not act as a direct risk factor for quality of life. In contrast, depression symptoms were shown to act as the significant overall risk factor for insomnia, fatigue symptoms, and quality of life. Furthermore, pain scores were correlated with other self-reported indices; however, it was not a direct risk factor for cancer-related fatigue. Precautions are required when interpreting this result because most patients who participated in this study did not report pain as the main symptom when visiting our Clinic. Pain scores were not significantly different between patients with high and low quality of life scores.
The results in this study that illustrated that cancer-related fatigue do not act as a direct risk factor on the quality of life in patients is in contrast to previous studies [25]; however, these results should be interpreted cautiously. First, there are the limitations to the Fatigue NRS used in this study because it displays the extent of fatigue that the patient experiences subjectively rather than being an objective index of cancer-related fatigue. Nonetheless, it is advantageous in a clinical setting because it generates a specific and definitive assessment for the cancer patient’s fatigue symptoms using a single question assessment. Therefore, the development of clinical indices or assessment tools that can more objectively reflect patients’ fatigue symptoms is important for future studies.
2. Relationship between cancer-related fatigue and TIB/d, and the effect of depression symptoms on quality of life
Next, we performed a pathway analysis using TIB/d as the dependent variable. We hypothesized that this more objectively reflected cancer-related fatigue symptoms than the Fatigue NRS. This analysis confirmed that cancer-related fatigue (as measured by TIB/d) is not a direct risk factor for the quality of life. However, this could also suggest that TIB/d cannot be used as an objective index to represent fatigue symptoms.
Accordingly TIB/d did not display significant correlation with fatigue symptoms. In contrast, we confirmed that depression symptoms are a risk factor for increased TIB/d. These data are in line with previous studies showing that depression symptoms are associated with reduced daytime activities [26]. Taken together, these results cannot confirm whether all fatigue symptoms and TIB/d were direct risk factors for reduced quality of life in patients with cancer. Nonetheless, interpretation of the results should be considered carefully because of the limitations of the Fatigue NRS. Furthermore, TIB/d may not be an appropriate index to objectively reflect fatigue symptoms in patients with cancer. Therefore, an objective assessment tool for fatigue symptoms cancer patients should be developed for future studies.
The pathway analysis revealed that depression symptoms in patients with cancer have an overall effect on quality of life, insomnia, fatigue symptoms, and a reduction in the daytime activities. Another pathway analysis was executed for each of the groups with depression symptoms that are above (PHQ-9 score, > 9) or below (PHQ-9 score, ≤ 9) the cutoff-point. This analysis confirmed that fatigue symptoms remain in the patient group without depression and interact with insomnia and dysfunctional beliefs about sleep. Interestingly, the effects of the fatigue symptoms were not present in the patient group with depression together with a marked reduction in the daytime activities.
We hypothesized that this is caused by depression overwhelming the fatigue symptoms, which causes a masking effect on the interaction among other factors. This is consistent with the results of existing studies showing that depression symptoms impart a greater influence on quality of life in cancer patients [27,28]. Therefore, assessment and therapeutic intervention of the depression symptoms in patients with cancer would lead to more effective outcomes in improving patients’ quality of life. However, we should consider that cancer patients suffer from depression frequently with fatigue, insomnia, or anxiety as co-morbidities simultaneously [29]. Sometime, it is not easy to discriminate those symptoms, and we should manage those symptoms at the same time. In this study we tried assessing each symptom separately using specific rating scales, and exploring which symptom is most powerful predictor for patients’ quality of life. In clinical practice, it is needed to measure and manage patients’ various psychiatric symptoms for improving cancer patients’ quality of life.
There are some limitations of this study. First, the analysis was executed within the patients with cancer alone; therefore, comparative analysis with a normal control group was not executed. Furthermore, this was a retrospective cross-sectional study via review of medical records; therefore, precautions are necessary in the interpretation of causal relationships among the relevant factors. Second, the total number of patients in this study was low and insufficient to execute various subordinate group analyses. Females accounted for the majority of patients and breast cancer accounted for more than half of the types of the cancers included in this study. Therefore, generalizing and applying the results of the analyses to the entire population should be undertaken cautiously. Third, the results in this retrospective medical record review study cannot be generalized into all cancer patients. This study was performed in a single hospital despite the center. In addition, in this study over half of subjects were breast cancer patients, but other various types of cancers were also included. We can speculate that the influence of patients’ depression or cancer-related fatigue on their quality of life can be varied in different cancer types. However, we could not perform subgroup analysis in each individual cancer type. Fourth, in this study, we could not consider other physical symptoms which were reported to be related with cancer patients’ quality of life such as nausea, vomiting, hot flushes, or alopecia. Finally, the use of more objective assessment tools, such as more accurate fatigue measures and records on the movement activities via Actigraphy or Polysomnography would have provided more accurate information on the cancer-related fatigue, sleep states, or daytime activities.
In conclusion, we confirmed that cancer-related fatigue is a common and painful side effect experienced by patients with cancer during treatment. Furthermore, depression, anxiety, insomnia, and dysfunctional thinking on sleep can act as risk factors for cancer-related fatigue. Interestingly, cancer-related fatigue itself does not act as a direct risk factor for quality of life; however, a cautious interpretation of the results is required because of limitations in the assessment tools for measuring fatigue symptoms. Accordingly, the development of assessment tool specific for cancer-related fatigue would be important for future studies. Additionally, we confirmed that depression symptoms act as an important risk factor in the quality of life of patients with cancer.
Notes
Ethical Statement
This study was performed with the approval of the Institutional Review Board (IRB) of Asan Medical Center (IRB Approval No. 2020-0153). Obtaining informed consent was waived by the IRB, since this study was retrospective medical records review study.
Author Contributions
Conceived and designed the analysis: Yeo S, Lee J, Kim K, Kim HJ, Chung S.
Collected the data: Yeo S, Chung S.
Contributed data or analysis tools: Yeo S, Kim HJ, Chung S.
Performed the analysis: Kim HJ, Chung S.
Wrote the paper: Yeo S.
Conflicts of Interest
Conflict of interest relevant to this article was not reported.