Changes in the Diagnostic Efficiency of Thyroid Fine-Needle Aspiration Biopsy during the Era of Increased Thyroid Cancer Screening in Korea
Article information
Abstract
Purpose
The volume of thyroid cancer screening and subsequent thyroid fine-needle aspiration (FNA) have rapidly increased in South Korea. We analyzed the thyroid cancer diagnoses/thyroid FNA ratio according to the annual number of FNA to evaluate changes in the diagnosticefficiency of FNA.
Materials and Methods
This was a nationwide population-based retrospective cohort study. The overall thyroid cancer diagnoses/thyroid FNA ratio and annual incremental thyroid cancer diagnoses/incremental thyroid FNA ratio were indirectly calculated using data obtained from the Korea Central Cancer Registry database and the Korean National Health Insurance Service claims database from 2004 to 2012. Pearson correlation analyses were performed to evaluate the strength of linear associations between variables.
Results
The number of thyroid FNA increased from 28,596 to 177,805 (6.2-fold increase) from 2004 to 2012. The overall thyroid cancer diagnoses/thyroid FNA ratio decreased from 36.5% in 2004 to 25.1% in 2012 and was negatively correlated to the number of FNA (R=‒0.977, p < 0.001). The annual incremental thyroid cancer diagnoses/incremental thyroid FNA ratios (range, 15.3% to 30.7%) were always lower than the overall thyroid cancer diagnoses/thyroid FNA ratio in each year and also worsened according to the increase in the number of FNA (R=‒0.853, p=0.007).
Conclusion
The diagnostic performance of both overall and annual incremental thyroid FNA worsened, whereas the number of thyroid FNA procedures increased. More sophisticated indications for FNA are required to improve its diagnostic efficiency, considering the increased burden of screening-detected thyroid nodules.
Introduction
The incidence of thyroid cancer has significantly increased over the past two decades worldwide [1]. Several studies have shown that the increased implementation of various imaging modalities has contributed to the increasing diagnoses of thyroid cancer [1-5]. This phenomenon is particularly remarkable in the Republic of Korea, where the incidence of thyroid cancer has increased nearly by 10-fold from 1999 to 2013 [6].
Thyroid fine-needle aspiration (FNA) is the most important diagnostic test for detecting thyroid cancer [7]. Regarding the rapid increase in thyroid cancer, there is a growing concern that the number of FNA procedures has unnecessarily increased [8,9]. If FNA is performed unnecessarily in screening-detected thyroid nodules that have a low likelihood of cancer, the relative frequency of obtaining negative results could increase, and the diagnostic efficiency of FNA might decrease according to the increased volume of screening and subsequent FNA.
The diagnostic efficiency of a test may be assessed using the number of diagnoses of the index disease compared to the number of tests performed [10-14]. If the frequency of detecting a patient according to the test is reduced, the number of tests required to identify one patient would increase, resulting in an increase in the overall cost and potential adverse events [10-14]. Therefore, the diagnostic efficiency of FNA could be estimated using the ratio of thyroid cancer diagnoses and FNA procedures.
We assumed that the question of whether FNA for the diagnosis of thyroid cancer was performed efficiently could be answered by looking at recent changes in the ratio of thyroid cancer diagnoses and FNA procedures. In addition, we assumed that the ratio of incremental thyroid cancer diagnoses and incremental thyroid FNA biopsies would reflect the diagnostic efficiency of FNA for additionally detected thyroid nodules from the increased screening. Thus, to evaluate the change of diagnostic efficiency of FNA and the potential influence of the number of FNA biopsies to the changed efficacy, we analyzed the changes in overall and annual incremental thyroid cancer diagnoses/thyroid FNA ratio according to the annual number of FNA biopsies performed during the era of increased thyroid cancer screening in South Korea.
Materials and Methods
1. Data sources
This was a nationwide retrospective cohort study from 2004 to 2012 using two nationwide databases.
The number of thyroid FNA biopsies performed was obtained from the claims database of the National Health Insurance (NHI) system of the Republic of Korea [15]. The NHI system is a mandatory universal health insurance system that has been covering the entire population (> 50 million) in Korea since 1989. NHI covers all forms of health services, including admission, ambulatory care, and pharmaceutical services. The medical claims database stores data about the use of all healthcare services. Moreover, it contains extensive data, including demographic information such as age and sex, record of medical services such as diagnosis statements according to the International Classification of Diseases, 10th revision (ICD-10), detailed statements about prescriptions and surgical and other procedures such as thyroid FNA.
We used the Korea Central Cancer Registry (KCCR) database to obtain the data regarding thyroid cancer diagnoses [16]. The KCCR was initiated by the Ministry of Health and Welfare in Korea in 1980 and then expanded nationally to cover over 95% of all patients with newly diagnosed cancer in Korea during the study period.
2. Case identification
The information about the number of FNA biopsies was identified using the NHI claims code (C8591) in the NHI claims database. The number of thyroid FNA biopsies according to sex was obtained only from 2006 as claims data for thyroid FNA until 2005 were often missing sex information. The number of newly diagnosed patients with thyroid cancer was obtained from the KCCR database from 2004 to 2012.
3. Overall thyroid cancer diagnoses/thyroid FNA ratio
We considered that most thyroid FNA were performed to diagnose thyroid cancer, and most patients diagnosed with thyroid cancer underwent preoperative thyroid FNA. Since the NHI claims database can store all data on thyroid FNA performed in the Republic of Korea, the nationwide thyroid cancer diagnoses/thyroid FNA ratio could be indirectly estimated by dividing the number of incident cases of thyroid cancer in a year by the number of thyroid FNA in such year.
4. Annual incremental thyroid cancer diagnoses/incremental thyroid FNA ratio
The annual increment of thyroid cancer diagnoses was calculated as the number of thyroid cancer diagnoses in each year minus the number of thyroid cancer diagnosis in the preceding year (e.g., annual increment of thyroid cancer diagnoses in 2010=the number of thyroid cancer diagnoses in 2010‒the number of thyroid cancer diagnoses in 2009). The annual increment of thyroid FNA biopsies for each year was calculated as the number of thyroid FNA biopsies in each year minus the number of thyroid FNA biopsies in the preceding year (e.g., annual increment of thyroid FNA biopsies in 2010=the number of thyroid FNA biopsies in 2010–the number of thyroid FNA biopsies in 2009). The annual incremental thyroid cancer diagnoses/incremental thyroid FNA ratio was defined as the annual increment of thyroid cancer diagnoses divided by the annual increment of thyroid FNA biopsies.
5. Statistical analysis
Pearson correlation coefficients were calculated to evaluate whether the number of thyroid cancer diagnoses and the thyroid cancer diagnoses/thyroid FNA ratio were linearly associated with the annual number of FNA. All statistical analyses were performed using the Statistical Package for the Social Sciences software ver. 23.0 for Windows (IBM Corp., Armonk, NY). All tests were two-sided, and a p-value of < 0.05 was considered statistically significant.
6. Ethical statement
Personal identifiable information in the medical records was de-identified to comply with the Health Insurance Portability and Accountability Act privacy rule. In addition, since the information in the NHI database is encrypted, the database does not contain personal identifiers. The study was approved by the Institutional Review Board of Ilsan Hospital (IRB No. NHIMC 2016-02-007) and performed in accordance with the principles of the Declaration of Helsinki. The informed consent was waived.
Results
1. Number of annual thyroid FNA and thyroid cancer diagnoses
Table 1 shows the number of thyroid FNA and thyroid cancer diagnoses from 2004 to 2012. The number of thyroid FNA increased from 28,596 to 177,805 (6.2-fold increase) from 2004 to 2012. During the same period, the number of newly diagnosed patients with thyroid cancer increased from 10,424 to 44,621 (4.3-fold increase). A strong positive linear correlation was observed between the number of thyroid FNA and the number of thyroid cancer diagnoses (R=0.995, p < 0.001) (Fig. 1A).

Number of thyroid FNA and thyroid cancer diagnoses, and estimated thyroid cancer diagnoses/thyroid FNA ratio
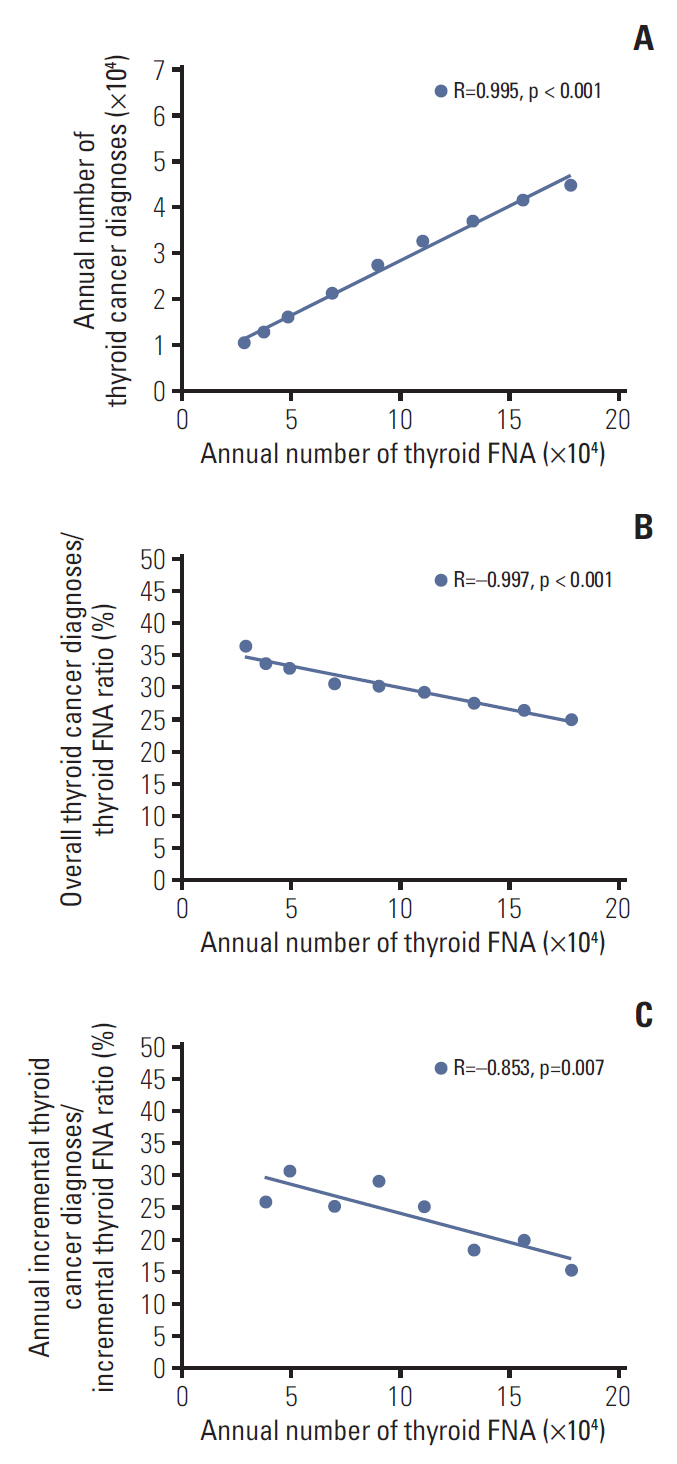
Pearson correlation coefficients were calculated to evaluate the association between the annual number of thyroid fine-needle aspiration (FNA) and the annual number of thyroid cancer diagnoses (A), overall thyroid cancer diagnoses/thyroid FNA ratio (B), and annual incremental thyroid cancer diagnoses/incremental thyroid FNA ratio (C). The lines indicate significant correlations (p < .05).
2. Overall thyroid cancer diagnoses/thyroid FNA ratio according to the passage of time and number of FNA
The overall thyroid cancer diagnoses/thyroid FNA ratio gradually decreased for 8 years from 36.5% in 2004 to 25.1% in 2012 (Table 1). A strong negative correlation was observed between the number of thyroid FNA and the overall thyroid cancer diagnoses/thyroid FNA ratio (R=–0.977, p < 0.001) (Fig. 1B).
3. Annual incremental thyroid cancer diagnoses/incremental thyroid FNA ratio according to the passage of time and number of FNA
Table 2 shows the incremental number of FNA, increment in thyroid cancer diagnoses, and annual incremental thyroid cancer diagnoses/incremental thyroid FNA ratio (which were assumed to reflect FNA for screening-detected thyroid nodule) from 2005 to 2012. A negative correlation was observed between the number of thyroid FNA biopsies and the annual incremental thyroid cancer diagnoses/incremental thyroid FNA ratio (R=–0.853, p=0.007) (Fig. 1C). During the entire research period, each annual incremental thyroid cancer diagnoses/incremental thyroid FNA ratio was lower than the overall thyroid cancer diagnoses/thyroid FNA ratio in the same year.
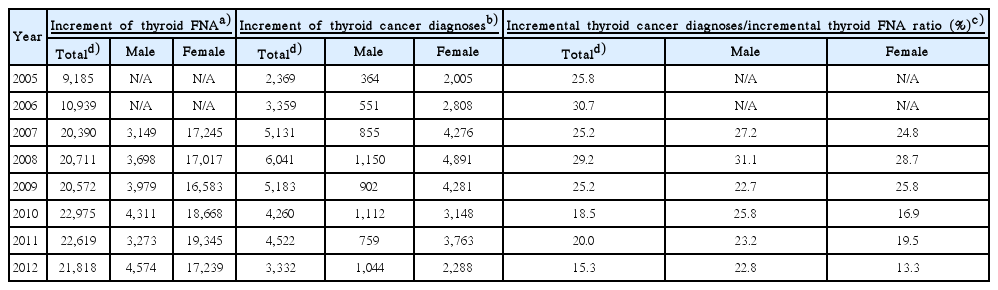
Estimated incremental thyroid cancer diagnoses/incremental thyroid FNA ratio
Discussion
In this study, we showed that the diagnostic efficiency of the overall and annual incremental thyroid FNA estimated by the thyroid cancer diagnoses/thyroid FNA ratio decreased as the annual number of thyroid FNA increased from 2004 to 2012.
The rapid increase in the incidence of thyroid cancer is largely attributed to the increase in thyroid cancer screening [1-5]. Udelsman and Zhang [2] showed a linear correlation between the frequency of neck ultrasonography and the incidence of thyroid cancer in the United States. Similar linear correlations were observed between the annual number of computed tomography imaging and incidence of thyroid cancer [3]. In addition, imaging procedures, such as Doppler examinations of the neck vessels and positron emission tomography scans, have increased the detection of incidental thyroid nodules [17,18]. As most of the nodules found in screening are confirmed as benign [19], many experts are concerned that increased thyroid cancer screening may lead to an increase in unnecessary FNA biopsies and a decrease in the diagnostic efficiency of FNA [20].
In this study, the number of thyroid FNA biopsies was positively correlated with the number of thyroid cancer diagnoses. However, the overall thyroid cancer diagnoses/thyroid FNA ratio decreased as the annual number of FNA increased. Our findings are in line with previous studies. In a study using U.S. Veterans Affairs administrative data from 2000 to 2012, the authors suggested that the increased thyroid cancer incidence may be related to increased use of thyroid ultrasound and FNA, based on their simultaneous increase [9]. Notably, the use of FNA increased much more rapidly than the incidence of thyroid cancer in the study, and the incidence increased only 2-fold while the use of FNA increased 7-fold [9]. In another study using an NHI sample cohort that includes approximately 2.2% of the entire Korean population, a higher frequency of thyroid FNA in a region was associated with a lower possibility of thyroid cancer diagnosis in patients who underwent thyroid FNA in the region [20]. Altogether, the diagnostic efficiency of FNA seems to be decreased when the frequency of thyroid FNA biopsies increases.
To further explore the cause of the decline in the diagnostic efficiency of FNA, we assumed that the incremental thyroid cancer diagnoses/incremental thyroid FNA ratio would indirectly reflect the diagnostic efficiency of FNA for additionally detected thyroid nodules from the increased screening. If the increase in the number of FNA biopsies and thyroid cancer diagnoses is largely attributed to the increase in the frequency of screening, the increment of thyroid FNA would reflect the number of FNA biopsies performed for additionally detected nodules from the increase in the frequency of screening (i.e., additional screening-detected thyroid nodules). In addition, the increment of thyroid cancer diagnoses would reflect the number of cancer diagnoses from the additional screening-detected thyroid nodules. We found that the annual incremental thyroid cancer diagnoses/incremental thyroid FNA ratio was lower than the overall thyroid cancer diagnoses/thyroid FNA ratio in each year. Moreover, the annual incremental thyroid cancer diagnoses/incremental thyroid FNA ratio decreased as the annual number of FNA biopsies increased. Therefore, the efficiency of the overall thyroid FNA appears to have been compromised during the period of increasing thyroid cancer screening as the diagnostic efficiency of FNA for screening-detected nodules was low and had decreased gradually. Our estimates of the annual incremental thyroid cancer diagnoses/incremental thyroid FNA ratio (range, 15.3% to 30.7%) are in accordance with the thyroid cancer diagnoses/thyroid FNA ratio in screening-detected nodules obtained by another study in Korea. In the study from a single institution, 111 cases of ultrasound-guided FNA were performed in the process of identifying 29 thyroid cancers from screening-detected thyroid nodules (thyroid cancer diagnoses/thyroid FNA ratio, 26.1%) [19].
Although thyroid FNA is relatively safe and inexpensive ($250 in the Republic of Korea and $500 in the United States [21,22]), the survival benefit of thyroid cancer screening program was low or even unclear [23,24]. A low diagnostic efficiency increases the number of FNA performed in the course of diagnosing a patient; thereby, it could increase the risk compared to the benefit of the test. Thus, the higher the number of screening-detected thyroid nodules, the higher the need for more sophisticated indications for FNA to improve its diagnostic efficiency and the balance between the risks and benefits.
This study has several strengths. First, this is the largest study to date of the relationship between FNA frequency and the number of thyroid cancer diagnoses using the NHI database including the entire Korean population. Second, to the best of our knowledge, this is the first study that suggests the worsened performance of FNA in screening-detected nodule caused by the increase in the frequency of FNA biopsies. Third, we overcame the limitations of the NHI database on the accuracy of diagnosis by using the KCCR database to assess the number of patients with thyroid cancer. Diagnostic accuracy is a common limitation in using health administrative data, although the reliability of the information in the NHI database has been previously validated in several studies [25-29].
This study also has several limitations. First, the number of patients with newly diagnosed thyroid cancer in this study may be slightly underestimated. The KCCR data are usually based on postoperative pathology results. Therefore, some patients with thyroid cancer who were followed up without surgery after FNA (active surveillance or inappropriate condition for operation) may be missing in this study. Second, there may be cases in which thyroid FNA was used for purposes other than the diagnosis of thyroid cancer and thyroid cancer was diagnosed without thyroid FNA. However, the diagnosis of thyroid cancer without performing FNA is rare. Third, several technological advances related to thyroid FNA, as well as training level and case volume of physicians, may influence the diagnostic efficiency of thyroid FNA [30-32]. However, the training level and case volume of physicians are likely to be enhanced according to the increased nationwide frequency of thyroid FNA, which would potentially improve diagnostic accuracy, just as the technological advances would. Our results suggest that the diagnostic efficiency of FNA was compromised despite the potential enhancement of its accuracy. Fourth, the exact volume of thyroid cancer screening could not be assessed since NHI did not cover thyroid ultrasonography during the study period. Thyroid cancer screening during the study period was often performed via a health screening program that was not covered by NHI. Thus, the diagnostic efficiency of FNA for screening-detected nodules was indirectly estimated based on several assumptions, even though the estimate was similar to the results obtained in the other study. Fifth, we could not determine the characteristics of the nodules targeted by FNA because of the absence of information about sonographic findings in the NHI database.
In conclusion, the overall diagnostic efficiency of FNA worsened according to the increase in the number of FNA, with a low and decreased diagnostic efficiency of incremental FNA. Our findings suggest that more sophisticated indications for FNA are required to improve its diagnostic efficiency, considering the burden of screening-detected thyroid nodules.
Notes
Conflict of interest relevant to this article was not reported.
Acknowledgements
The authors express their gratitude to Hyunsun Lim (Research Institute, National Health Insurance Service Ilsan Hospital) for providing statistical advice.
This study used the health administration data of the policy report published by National Health Insurance Service Ilsan Hospital (NHIS-2014-1-022).