Utility of the National Lung Screening Trial Criteria for Estimation of Lung Cancer in the Korean Population
Article information
Abstract
Purpose
Screening forlung cancerin high-risk patients using the National Lung Screening Trial (NLST) criteria resulted in a decreased lung cancer-related mortality rate. However, whether these criteria are applicable to the Korean has not been investigated thus far. Therefore, we estimated the utility of the NLST criteria as a screening tool for lung cancer in the Korean population.
Materials and Methods
The total number of newly diagnosed lung cancer cases in 2013 was obtained from the Korea National Statistical Office. The proportion of newly diagnosed lung cancer cases that met the NLST criteria was calculated via a retrospective cohort of a tertiary referral hospital. We estimated the nationwide proportion of patients who met the NLST criteria using the 5th Korea National Health and Nutrition Examination Survey conducted during 2010-2012 (KNHANES V).
Results
Using KNHANES V data, we found that approximately 6.92% of the general population of Korea would meet the NLST criteria. In the tertiary referral hospital, 29.6% of the 2,689 newly diagnosed lung cancer patients met the NLST criteria. In 2013, the total number of newly diagnosed lung cancer cases in Korea was 23,177. The estimated nationwide proportions of lung cancer patients who met and did not meet the NLST criteria were 0.37% and 0.06%, respectively, yielding a ratio of 5.78.
Conclusion
The NLST criteria demonstrated sound clinical utility for lung cancer screening of high-risk patients in Korea.
Introduction
According to the Global Burden of Cancer Study 2012, lung cancer is a common cancer (1.8 million cases) and the number one cause of cancer-related deaths, and accounts for 1.6 million cases worldwide owing to a high case fatality rate (0.87; overall ratio of mortality to incidence) [1,2]. Furthermore, the 5-year survival rate for lung cancer does not vary drastically across stages and has remained consistently low over the past several decades, because the majority of patients are diagnosed at an advanced stage [3]. Therefore, early detection of lung cancer is important to improve survival rates. For the purpose of early detection of lung cancer, large-scale clinical trials of lung cancer screening methods, such as chest radiography (CXR) and sputum cytology, have been conducted. However, these trials did not demonstrate the reduction of lung cancer mortality rate [4]. Before the National Lung Screening Trial (NLST), lung cancer screening was not recommended [5]. In 2011, the NLST showed a 20% reduction in lung cancer mortality rates and a 6.7% decrease in all-cause mortality rates [6]. This positive result of NLST could be explained by the following two reasons. First, they used low-dose chest computed tomography (LDCT) which is higher sensitivity than CXR as screening tools. Performing additional diagnostic procedures resulted in a higher detection rate of early-stage lung cancers in the LDCT group than in the CXR group; thus, a lower mortality rate was observed in the LDCT group [7]. Second, the NLST selected participants with high risk based on age and cumulative tobacco smoke exposure. Thus far, the NLST has influenced many guidelines for lung cancer screening, including those drafted by the National Comprehensive Cancer Network, American Association for Thoracic Surgery, American Colleges of Chest Physicians, American Society of Clinical Oncology, and U.S. Preventive Services Task Force [8-11]. Most current screening guidelines have been adopted from the NLST criteria itself.
In Korea, the National Cancer Information Center has been recommending lung cancer screening for people who meet the NLST criteria since 2015 [12] and based on this recommendation the Ministry of Health and Welfare established a nationwide lung cancer screening pilot study in 2017 [13]. However, the validity of the NLST criteria has not been evaluated in the Korean population thus far. Therefore, the aim of the present study was to investigate the utility of the NLST criteria for lung cancer screening in the Korean population.
Materials and Methods
1. Study design and participants
To estimate the proportion of individuals among the Korean population who met the NLST criteria, we used two data sets from the 5th Korea National Health and Nutrition Examination Survey (KNHANES V) database. The KNHANES V was conducted over 2010-2012 by the Korean Centers for Disease Control and Prevention. It is considered to be representative of the health status in Korea. These data consist of responses from the Nutrition Survey, Health Examination Survey, and Health Interview Survey, and contain smoking history including current smoking status and the pack-year history of smoking. However, the KNHANES V does not provide valid information regarding when an ex-smoker quit smoking. Consequently, if an ex-smoker satisfied the age and smoking pack-year criteria, they were considered to have met the NLST criteria.
We also analyzed the medical records of enrolled patients who were diagnosed with lung cancer in the Seoul National University Hospital (SNUH) from 1 June 2012 to 31 December 2015. These patients were divided into two groups: an NLST-positive group, defined as patients who satisfied all the NLST eligibility criteria (age 55-74 years, a smoking history of at least 30 pack-years, and currently smoking or quit smoking within the past 15 years) [6], and an NLST-negative group, defined as patients who did not meet any of the criteria. Lung cancer stage was evaluated according to the 7th edition of the TNM classification [14].
Weighted analysis was used to analyze the KNHANES V data. All statistical analyses were performed using STATA ver. 13 (STATA Corp., College Station, TX). The level of statistical significance was set at p=0.05.
2. Ethical statement
The study was approved by the Institutional Review Board of SNUH (IRB No. 1612-026-812) and performed in accordance with the principles of the Declaration of Helsinki. The informed consent was waived.
Results
Of the people included in the KNHANES V database, the data for 12,475 persons were included in the final analysis after excluding persons whose smoking histories were not investigated and those aged below 40 years (Fig. 1A). The mean age of the population was 55.8 years, and 6.9% satisfied the NLST criteria. Furthermore, the proportion of ever smokers and the mean smoking pack-year index was 43.9% and 23.8, respectively (Table 1).
(A) Flow diagram of study population (fifth Korea National Health and Nutrition Examination Survey [KNHANES V]). (B) Flow diagram of study population (Seoul National University Hospital [SNUH]). NLST, National Lung Screening Trial.
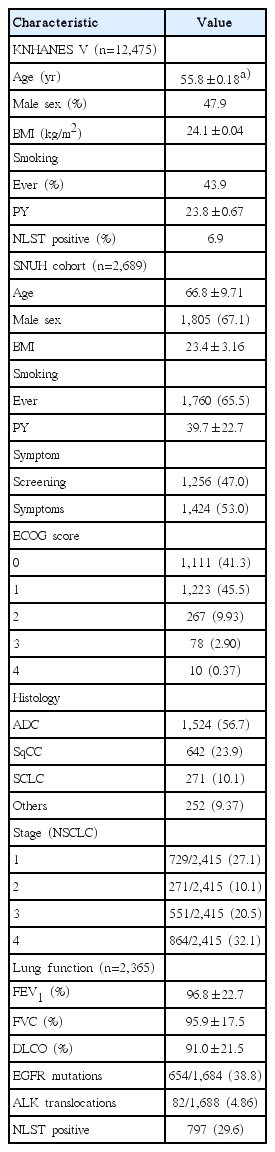
Baseline characteristics of the KNHANES V and SNUH cohort
At SNUH, we collected data for 2,725 patients and excluded 36 patients aged under 40 years (Fig. 1B). The mean age of this population was 66.8 years, and 29.6% of patients with lung cancer met the NLST criteria. The proportion of ever smokers (65.5%) was higher in the SNUH cohort than in the KNHANES V cohort (Table 1). The median follow-up period of the SNUH lung cancer patients was 1.49 years.
According to the Korea National Statistical Office, 23,177 people were diagnosed with lung cancer in 2013 [15,16]. Using SNUH lung cancer cohort data, we estimated that 6,860 (29.6%) and 16,317 (70.4%) lung cancer patients met and did not meet the NLST criteria, respectively. Using the KNHANES data we found that, of the Korean patients aged over 40 years, 1,893,065 (6.9%) satisfied the NLST criteria and 25,463,377 (93.1%) did not satisfy the NLST criteria. Therefore, among the patients who met the NLST criteria, about 0.37% (6,860/1,893,065) were estimated to have lung cancer, and conversely, about 0.064% (16,317/25,463,377) of people who did not satisfy the NLST criteria were expected to develop lung cancer. Importantly, the incidence of lung cancer was 5.58 times higher in the NLST-positive group (Fig. 2).
Estimation of lung cancer incidence in Koreans ≥ 40 years using National Lung Screening Trial (NLST) criteria. SNUH, Seoul National University Hospital; KNHANES V, fifth Korea National Health and Nutrition Examination Survey.
Discussion
The findings of our study showed that the incidence of lung cancer in Korea is 5.58 times higher among those who satisfy the NLST criteria than among those who do not. Thus far, no previous study has evaluated the utility of NLST criteria in the Korean population as a screening tool for high-risk patients.
Nonetheless, the application of the NLST criteria to the Korean population involves a few obstacles. Korea is a country with an intermediate tuberculosis incidence rate (80 cases per 1000,000 persons) [17]. In other words, the false-positive rate achieved via LDCT may be higher than that in countries enrolled in the NLST study. A high false positive rate was determined to be associated with cost effectiveness, health-related quality of life, or anxiety and other adverse events associated with invasive interventions such as biopsy. Therefore, a variety of approaches to reduce false-positive rate have been developed by increasing the threshold for pulmonary nodules, such as lung CT Screening Reporting and Data System [18].
Recently, ten Haaf et al. [19] demonstrated that both the sensitivities and specificities of the 6-year lung cancer incidence determined using the NLST criteria were lower than that reported using other screening criteria (e.g., Liverpool Lung Project or Bach model) in the Prostate, Lung, Colorectal and Ovarian Cancer Screening Trial CXR arm. Therefore, lung cancer screening in high-risk patients identified using NLST criteria will be helpful to develop a prediction model suitable for the Korean population.
Using KNHANES V data, we estimated that approximately 6.9% of the population in Korea would meet the NLST criteria. Previous studies have reported similar results: 6.2% of United States are covered among over 40 years population according to Surveillance, Epidemiology and End Result in the United States [20]. In addition, in this study, 29.6% of patients who were diagnosed with lung cancer met the NLST criteria. This result is also consistent with those of previous studies conducted in the United States and Asian population. Pinsky and Berg [20] reported that 26.7% of lung cancer patients in the United States met the strict NLST eligibility criteria using statistical models based on data derived from SEER. A total of 27.8% of lung cancer patients was covered in Asian population-based study [12].
There are several limitations in this study. First, the smoking history data in the KNHANES V was self-reported; therefore, it could have been underreported. Second, accurate estimation of lung cancer using the NLST criteria involves inevitable errors because the KNHANES V did not evaluate the participant’s history when they quit smoking. However, since the NLST-positive group identified using KNHANES V data contains not only the original NLST eligible population but also a larger proportion of people classified as NLST positive, the cancer incidence ratio would probably be higher than that estimated. Third, our results cannot be generalized to all Korean lung cancer patients because it used data obtained from a single tertiary hospital; moreover, the study was retrospective in nature. Nevertheless, the SNUH data cannot be regarded as unreliable because the NLST eligible population was similar to that described in previous studies conducted in other countries.
The benefits of lung cancer screening using LDCT might be more pronounced in Korean patients identified as being at high risk per the NLST criteria.
Notes
Conflict of interest relevant to this article was not reported.
Acknowledgements
This study was supported by a grant (No. 1612-026-812) from the SNUH Research Fund. The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.