Introduction
Liposarcoma (LPS) is a mesenchymal-origin cancer arising from precursors of adipocytes and accounts for 15% to 20% of all adult malignant soft-tissue sarcoma [1]. It can arise in any fat-containing region of the body, and is histologically classified into four subtypes; well-differentiated, dedifferentiated, myxoid/round and pleomorphic LPS [2]. Due to its rarity and the heterogeneity in tumor location and histology, the clinical characteristics, and oncologic outcomes of LPS, along with an appropriate proper treatment strategy for it, have not been well-established.
The mainstay of treatment for localized LPS is still surgical resection, but tumor recurrence is common even after surgery with curative intent. Other treatment modalities, including radiation therapy and systemic chemotherapy, are used in the multidisciplinary management of LPS. Radiation therapy has been recommended in soft-tissue sarcomas with large size, high-grade (especially myxoid subtype), positive resection margins, or extremity origin for better local control. However, its survival benefit remains unclear, and there is still no full consensus on the optimal indications for adjuvant radiation therapy in other histologic subtype or abdominal-pelvis LPS [3,4]. Conventional cytotoxic chemotherapy has different benefit based on histologic subtypes and anatomic sites of LPS. Patients with myxoid histology and extremity origin has known to be chemo-sensitive with a response rate of 40%–50% [5]. On the other hand, chemotherapy has limited efficacy in other histologic subtypes with a response rate of about 10% and is not generally recommended in the preoperative or postoperative setting [6–8]. Recently, it was suggested that immune-checkpoint inhibitors may have clinical activity for soft-tissue sarcomas in phase II trials that included patients with well-differentiated and dedifferentiated LPS [9,10]. However, it has not been comprehensively investigated whether the expression of programmed death-ligand 1 (PD-L1), one of the well-established predictors for response to immune-checkpoint inhibitors, is common in LPS and how PD-L1 positivity is related with patient outcome.
In the present single-center retrospective study, we aimed to determine the clinical course and treatment outcome of localized LPS and evaluate the expression level of PD-L1 and determine its relationship with clinical outcomes in well-differentiated and dedifferentiated LPS.
Materials and Methods
1. Patients
We retrospectively reviewed all consecutive patients who were treated for LPS at Asan Medical Center, Seoul, South Korea between July 1989 and January 2018 using the clinical database system of Asan Medical Center (Asan BiomedicaL Research Environment, ABLE) after extracting all records containing phrase “liposarcoma”. Patients whose diagnoses were not pathologically confirmed or whose electronic medical records were not available from initial diagnosis were excluded from the final analysis. Patients who had stage IV disease and did not receive curative-intent surgical resection were also not included. Clinical data regarding demographic factors, baseline tumor characteristics, treatment history and survival outcomes were retrospectively obtained by reviewing the anonymous records from ABLE.
Pathologic diagnosis of LPS and its histologic classification were made by expert sarcoma pathologists (K-J.C., J.S.S.) based on the World Health Organization (WHO) classification system. The treatment plan was decided on multidisciplinary approach at tertiary referral cancer in accordance with the international guidelines. Surgeons and radiologists determined the optimal extent of resection to achieve clear resection margin and to preserve the adjacent critical structures. Experienced medical oncologists and radiation oncologists determined the need of postoperative radiotherapy and chemotherapy, considering tumor location, tumor size, histologic subtype, grade, adjacent structures as well as resection margin status.
2. PD-L1 staining
When available, formalin fixed paraffin-embedded tumor samples collected from patients with well-differentiated and dedifferentiated LPS during a previous biopsy or surgery were reviewed by a designated pathologist and analyzed for PD-L1 expression. Immunohistochemical staining for PD-L1 was performed with the Ventana SP263 assay (rabbit monoclonal primary anti–PD-L1 antibody, Ventana Medical Systems, Tucson, AZ), Food and Drug Administration (FDA)-approved complementary diagnostics [11]), on the Benchmark XT staining systems and Ultra with the OptiView Universal DAB Detection Kit (Ventana Medical Systems), according to the manufacturer’s instructions. Whole tumor section was stained in each case to adequately reflect heterogeneity of expression. Positive PD-L1 expression was defined as staining in ≥ 1% of tumor cells.
3. Statistical analysis
Overall survival (OS) was defined as the time between the diagnosis and death from any cause. Recurrence-free survival (RFS) was defined as the duration between the resection with curative intent until tumor recurrence or death from any cause, whichever came first. When recurrence or death were not observed, survival time was censored at the date of the last follow-up visit. Survival outcomes were estimated using the Kaplan-Meier method and compared using the log-rank test. Multivariate analyses for survival outcomes were analyzed using the Cox proportional hazards model. A p-value less than 0.05 was considered statistically significant. Statistical package for the Social Sciences ver. 22.0 (IBM Corp., Armonk, NY) was used for all statistical analyses.
Results
Out of 467 patients identified from the database, 332 patients who had underwent curative-intent resection for pathologically-confirmed localized LPS and had sufficient medical records were finally included in this retrospective analysis and 135 patients were excluded for following reasons: medical records not available (n=71), diagnosed and treated at other institution (n=26), follow-up loss after diagnosis (n=24), distant metastasis at diagnosis (n=12), or no surgery due to high perioperative risk (n=2). Baseline characteristics of all patients evaluated in this study are summarized in Table 1. The median age of the patients was 56 years (range, 19 to 87 years) with males comprising 60.8% (202/332) of patients. The most common subtype was well-differentiated LPS (125/332, 37.7%), followed by dedifferentiated (103/332, 31.0%), myxoid/round (91/332, 27.4%), and pleomorphic (13/332, 3.9%). By primary site, abdomen-pelvis (158/332, 47.6%) was most frequently involved; extremity (136/332, 41.0%), thorax (22/332, 6.6%) and head-neck (16/332, 4.8%) came next.
1. Treatment and clinical outcomes
All included patients underwent curative-intent surgery as the first treatment for their localized LPS; no one received preoperative chemotherapy or radiotherapy. Information on treatment and recurrence is summarized in Table 1. The R0 resection rate was 57.2% (190/332), and about half (157/332, 47.3%) of patients underwent postoperative treatment consisting of radiotherapy (111/332, 33.4%), chemotherapy (17/332, 5.1%), or both (29/332, 8.7%). During a median follow-up duration of 81.2 months, recurrence was observed in 135 patients (40.7%) after surgery, and 86.7% (117/135) of recurrences were local. Recurrence pattern was slightly different between histologic subtypes. Dedifferentiated and pleomorphic LPS had relatively high recurrence rate (63.1% and 61.5%) compared with well-differentiated (30.4%) and myxoid/round (26.4%) LPS, but distant recurrence was consistently observed in less than 10% across all subtypes (S1 Table).
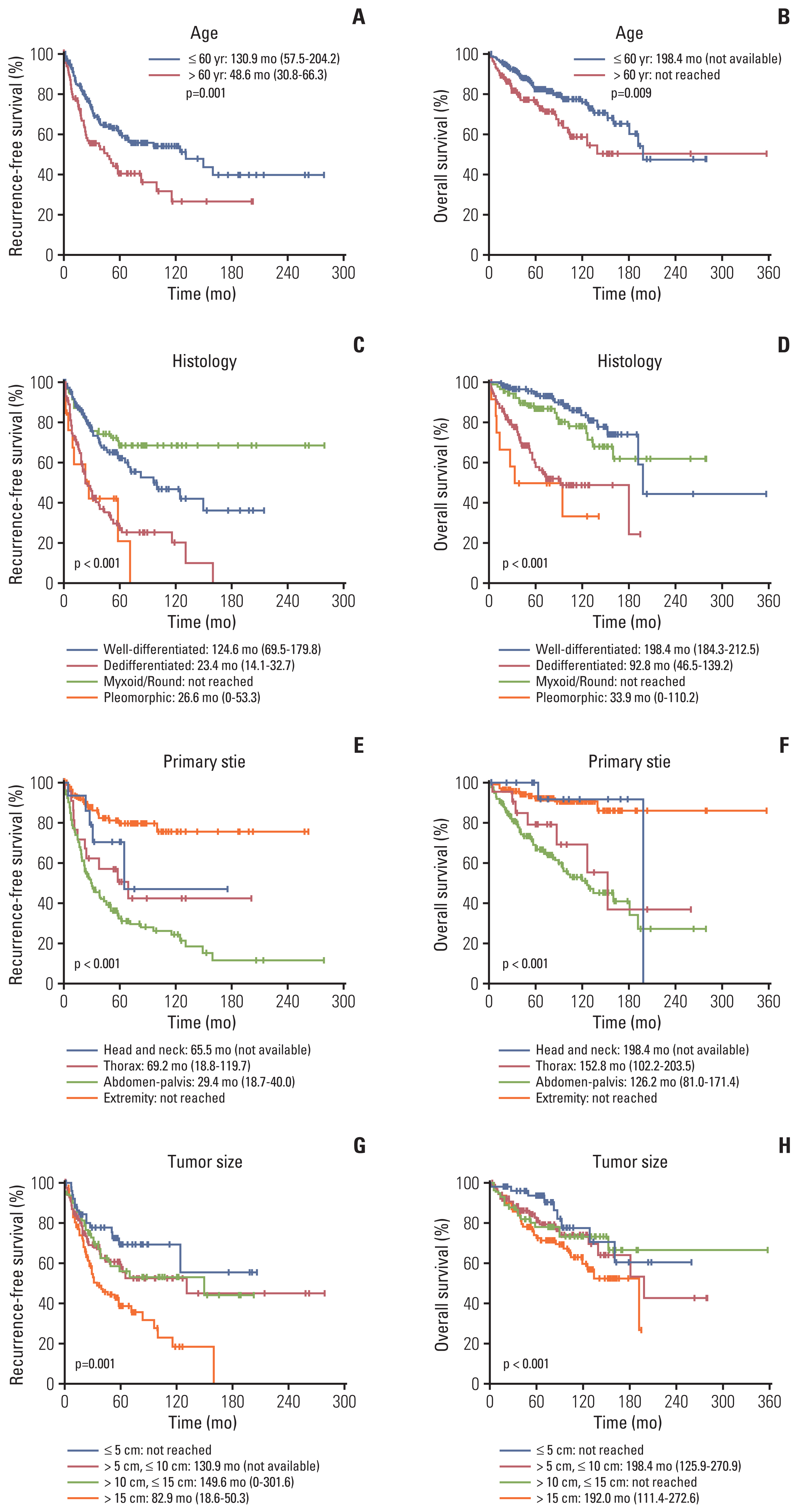
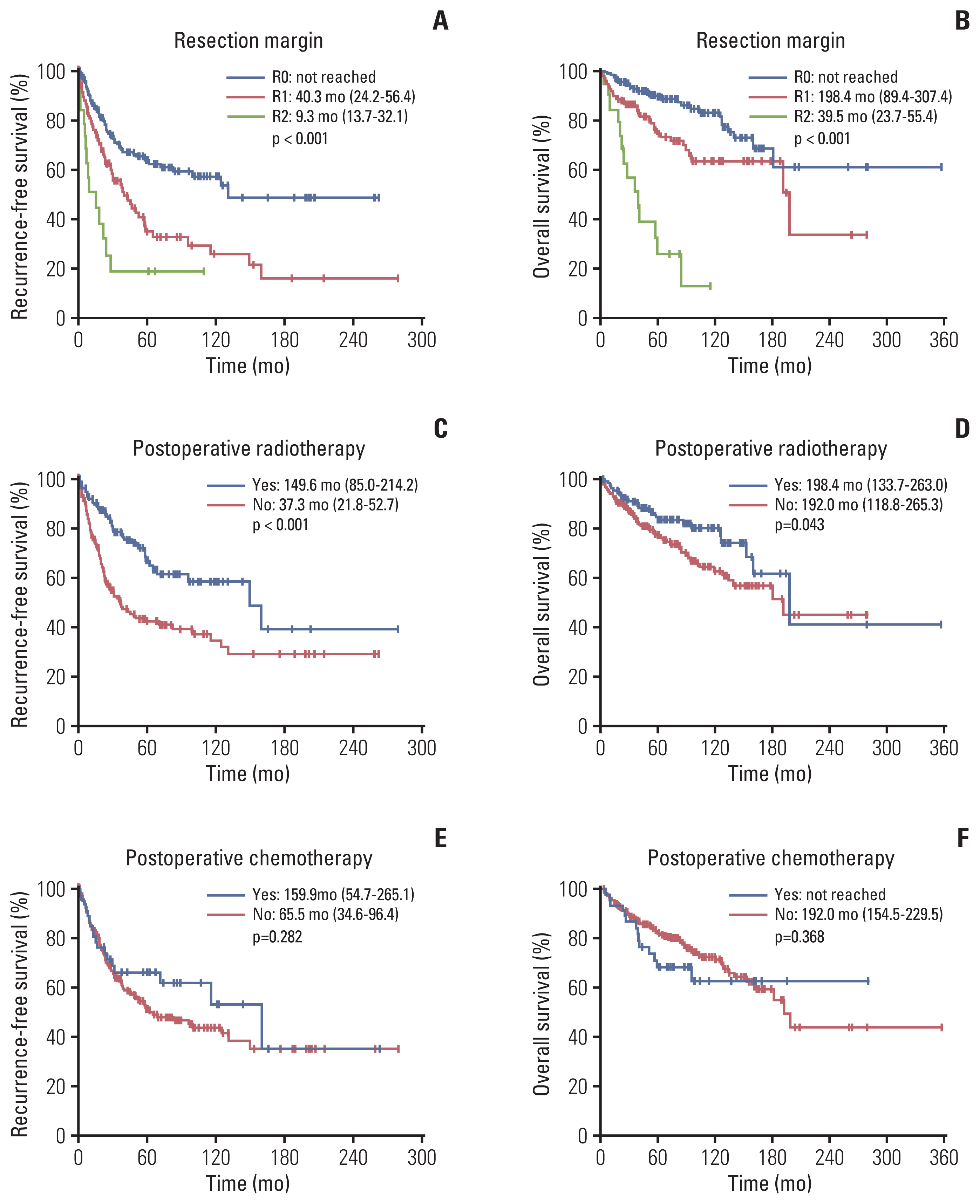
Median OS and RFS of the whole cohort were 198.4 (95% CI, not available) and 82.9 months (range, 46.9 to 118.8 months), respectively. Age > 60 years was significantly associated with poorer survival outcomes (vs. ≤ 60 years; median RFS, 48.6 vs. 130.9 months, p=0.001; median OS, 198.4 vs. not reached, p=0.009) (Fig. 1A and B). By histology, well-differentiated LPS (median RFS, 124.6 months; median OS, 198.4 months) and myxoid/round LPS (median RFS and OS, not reached) tended to have better prognosis than dedifferentiated LPS (median RFS, 23.4 months; median OS, 82.8 months) and pleomorphic LPS (median RFS, 26.6 months; median OS, 33.9 months) (Fig. 1C and D). LPS originating in the abdomen-pelvis (median RFS, 29.4 months; median OS, 126.2 months) had the poorest survival, while LPS originating in the extremity had most favorable survival (median RFS and OS, not reached) (Fig. 1E and F). Larger tumor was also associated with shorter RFS (≤ 5 cm vs. > 15 cm, not reached vs. 82.9 months, p=0.001) and OS (not reached vs. 192.0 months, p < 0.001) (Fig. 1G and H). Regarding treatment, resection margin status was key factor determining RFS (R0 vs. R1 vs. R2, not reached vs. 40.3 months vs. 9.3 months, p < 0.001) and OS (R0 vs. R1 vs. R2, not reached vs. 198.4 months vs. 39.5 months, p < 0.001) (Fig. 2A and B). Furthermore, adjuvant radiotherapy resulted in longer RFS (vs. no adjuvant radiotherapy; 149.6 months vs. 37.3 months, p < 0.001) but had less impact on extending OS (198.4 months vs. 192.0 months, p=0.043) (Fig. 2C and D). On the other hand, adjuvant chemotherapy tended to improve RFS (vs. no adjuvant chemotherapy; 159.9 months vs. 65.5 months, p=0.282) and OS (not reached vs. 192.0 months, p=0.368), but these differences were not statistically significance (Fig. 2E and F). In multivariate analysis, histology, primary site, resection margin status and postoperative radiotherapy remained significantly associated with RFS and OS, while age only remained significantly associated with OS (Table 2). Tumor size larger than 5 cm was associated with shorter RFS (hazard ratio [HR], 1.83) with marginal p-value of 0.046, but it was not led to the shortening of OS (not retained in multivariate analysis). When analyzed by primary site, positive microscopic resection margin status (R1 resection) was associated with shorter RFS and OS compared with clear resection margin (R0 resection) in abdomen-pelvis LPS, while it did not affect both RFS and OS in extremity LPS (S2 Fig.). Postoperative radiotherapy extended RFS and OS abdomen-pelvis LPS. In extremity LPS, it extended RFS, but longer RFS did not lead to better OS (S3 Fig.).
2. Abdominal-pelvis LPS
Among patients with localized LPS originating in the abdomen-pelvis (n=158), visceral involvement was observed in 31.0% (49/158), and 12.0% of patients (19/158) had multifocal disease. Visceral involvement, which was defined as microscopic or macroscopic tumor invasion into the adjacent organs such as kidney, colon, pancreas, liver, bladder, and adrenal grand, was associated with shorter RFS (vs. no visceral involvement, 18.2 months vs. 46.7 months, p < 0.001) and OS (56.3 months vs. 181.0 months, p < 0.001) (S4A and S4B Fig.). Compared with patients having a solitary abdomin-pelvic lesion, patients with multifocal disease had significantly poorer RFS (8.7 months vs. 34.4 months, p < 0.001) and OS (37.7 months vs. 128.3 months, p=0.002) (S4C and S4D Fig.). The negative prognostic impact of visceral involvement and multifocality remained significant in a multivariate analysis with age, histology, resection margin, and postoperative radiotherapy (S5 Table).
3. PD-L1 expression in localized LPS
A total of 149 patients who were pathologically diagnosed with well-differentiated (n=73) or dedifferentiated (n=76) LPS and had tissue available for immunohistochemical staining were included in this analysis for PD-L1 expression (Fig. 3A–C). The PD-L1 positive (tumor proportion score ≥ 1%) rate was 31.5% and 51.3% in well-differentiated and dedifferentiated LPS, respectively. There were no significant differences in baseline characteristics or treatment between the PD-L1 positive and negative group both in well-differentiated and dedifferentiated LPS (S6 Table).
Overall, PD-L1 expression did not have an impact on RFS (vs. no expression, median 34.4 months [95% confidence interval (CI), 24.0 to 44.9] vs. 37.4 months [95% CI, 16.5 to 58.2], p=0.602) and OS (vs. no expression, median not reached vs. 181.0 months [95% CI, 72.4 to 289.6], p=0.539) (Fig. 3D and E). A subgroup analysis was additionally performed by histologic type (S7 Fig.). In well-differentiated LPS, PD-L1 expression was associated with shorter RFS (vs. no expression, 31.3 months [95% CI, 23.5 to 39.2] vs. 99.8 months [95% CI, 63.4 to 136.2], p=0.023), which remained significant in the multivariate analysis (HR, 2.68 [95% CI, 1.10 to 6.55], p=0.030). In dedifferentiated LPS on the other hand, PD-L1 positive patients had longer RFS (vs. PD-L1 negative patients, 34.3 months [95% CI, 21.9 to 46.9] vs. 18.3 months [95% CI, 15.7 to 21.0], p=0.032), which showed statistical significance (HR, 0.46 [95% CI, 0.24 to 0.87]; p=0.017) in the multivariate analysis (Table 3). OS was not significantly different according to PD-L1 expression both in well-differentiated and dedifferentiated LPS.
Discussion
This single-center retrospective study described the long-term clinical courses of 332 localized LPS patients after surgery and evaluated prognostic factors for survival outcomes after curative-intent surgery. The most common histologic subtype and primary tumor site in this cohort were well-differentiated LPS (37.7%) and the abdomen-pelvis (47.6%), respectively. We found that age, histologic subtype, primary tumor site, resection margin status, and postoperative radiotherapy independently influenced the postoperative prognosis of LPS.
OS was well stratified by the histologic subtypes. OS for patients with well-differentiated were significantly longer compared with those with dedifferentiated and pleomorphic tumors and it was a significant independent factor affection in the multivariate analysis (HR for RFS 0.45, p < 0.001; HR for OS 0.30, p < 0.001). Our findings are consistent with prior reports that well-differentiated LPS have 5-year survival rates higher than 90%, while 5-year survival rates of pleomorphic or dedifferentiated variants ranges from 30%–70% [12].
Primary tumor site also had a significant impact on RFS and OS after adjusting for other prognostic factors in multivariate analysis. Patients with abdominal-pelvic LPS had the worst prognosis with a median RFS of 29.4 months and OS of 126.2 months, while those with extremity LPS showed the longest survivals (both RFS and OS not reached). Our results are in line with a prior large prospective cohort study of 801 patients which reported that primary tumor site is an independent predictor for 12-year disease specific survival in LPS (retroperitoneal vs. extremity LPS, 32%–53% vs. 82%–87%, χ2=19.01, p=0.0008) [13]. Although a recent single-center retrospective study in Germany stated that primary site was not associated with prognosis, this study may be limited because it included a relatively small number of patients (n=130), and extremity LPS accounted for more than 70% of study population [14]. In retroperitoneal LPS, contiguous organ involvement has been reported to be common (26%–48%) and to be associated with increased risk of recurrence [13,15]. In our study, visceral involvement was found in about a third of abdomen-pelvis LPS patients and was an additional independent prognostic factor (RFS: HR, 1.8; p=0.014; OS: HR, 2.40; p=0.005). Meanwhile, researchers from MD Anderson Cancer Center reported that multifocality was associated with worse OS in patients with retroperitoneal soft-tissue sarcoma of multiple histologies (5-year survival rate, 31% vs. 60%; p < 0.001) [16]. Here, we showed similar findings on the prognostic role of multifocality in LPS (RFS: HR, 3.97; p < 0.001; OS: HR, 2.44; p=0.025).
Regarding treatment, complete resection with clean microscopic margins is the utmost goal of treatment and the most important factor in predicting postoperative survival. Our finding that patients with positive resection margins had much worse outcomes (RFS: HR, 2.50; p < 0.001; OS: HR, 2.29; p=0.002) are concordant with such previous findings. It should be noted that clean microscopic margin status (R0 resection) prolonged both RFS and OS compared to microscopic tumor positive margin status (R1 resection) in abdomen-pelvis LPS, but microscopic margin status had no influence on RFS and OS in patients with extremity LPS. Unlike the importance of surgical resection, the benefits of using postoperative chemotherapy and radiation therapy remains controversial. In our study, adjuvant radiotherapy was associated with longer RFS (HR, 0.37; p < 0.001) and OS (HR, 0.57; p=0.029), while adjuvant chemotherapy showed no benefit to both RFS and OS. From the subgroup analysis, postoperative radiotherapy was associated with a longer RFS but not OS in extremity LPS, while patients with abdomen-pelvis LPS who received with postoperative radiotherapy had longer OS as well as RFS. One possible explanation is that lowering recurrence is more crucial for patients with abdomen-pelvis LPS because they are harder to treat with re-excision or radiotherapy due to the deep location of the tumor and its proximity to the vital organs.
Notably, our data suggest that PD-L1 is expressed in decent proportion of well-differentiated and dedifferentiated LPS, but its role as a prognostic biomarker is unclear, with conflicting results between well-differentiated and dedifferentiated histologic subtypes. It has been previously reported that PD-L1 positivity rate varies according to the histologic subtypes of sarcoma [17–24], and PD-L1 positive sarcomas tend to have poorer survival outcomes [17,19,21–24], as in other solid cancers. However, those studies were limited by much heterogeneity in histologic subtypes, and a small number of patients with LPS were included (Table 4). In the present study, we evaluated the PD-L1 status with FDA-approved SP263 assay in a larger population (73 with well-differentiated LPS and 78 with dedifferentiated LPS). Although optimal cutoff value for PD-L1 expression remains unclear, we chose > 1% as like in previous sarcoma studies listed in Table 4. Thirty-one point five percentage of well-differentiated and 51.3% of dedifferentiated LPS patients were positive for PD-L1 expression, which is rather higher than former reports. The impact of PD-L1 positivity on prognosis was inconsistent between histologic subgroups in our study. Some researchers studied tumor-infiltrating lymphocytes, programmed cell death protein 1/PD-L1 expression, and tertiary lymphoid structures in LPS tissue, and showed that immune microenvironment of LPS is heterogeneous according to histologic subtypes, tumor grade, tumor size, multifocality, and primary or recurrent status [22,25]. The studies suggested Immunotherapy might have the potential for efficacy in a subset of LPS and there have been phase II trials (SARC028 and ALLIANCE) showing the potential activity of anti–PD-L1 therapies in soft-tissue sarcoma patients [9,10], and several clinical trials of immune-oncology agents and biomarker studies are ongoing [26,27]. Further studies are needed to evaluate the clinical implications of PD-L1 status as well as other biomarkers including presence of tertiary lymphoid structures and distribution of tumor-infiltrating lymphocytes in LPS. Those studies are expected to play an important role in solving the unmet needs in immunotherapeutic strategies for advanced LPS.
This study is limited by its retrospective nature, but we tried to minimize selection bias and demonstrate real-world clinical data by including all patients diagnosed with LPS. Also, although changes in the multidisciplinary management of LPS and pathologic diagnosis may have occurred over the study period, we inevitably had to include less recent patients due to the rarity of LPS. However, those limitations may be mitigated by the fact that in this study, the pathologic diagnosis of LPS and its histologic classification were confirmed by a dedicated sarcoma pathologist and treatment decisions were made in relatively good accordance with guidelines by a multidisciplinary team at an academic tertiary center.
In conclusion, our result showed that the clinical course of LPS is heterogeneous according to its histologic subtype and primary tumor site. We also suggest that R0 resection is important to lower recurrence rates and adjuvant radiation therapy may provide additional benefit following surgical resection in patients with localized LPS. Also, a decent portion of well-differentiated and dedifferentiated liposarcomas were positive for PD-L1 expression, but its prognostic impact was not clear. Further research in a larger population is needed to determine the clinical implications of PD-L1 expression and the role of immune-checkpoint inhibitors in advanced-stage LPS, which has limited therapeutic options.