INTRODUCTION
Renal cell carcinoma (RCC) can metastasize to almost any organ, but metastasis to the small bowel is rare. Small bowel metastasis from RCC may induce obstruction, bleeding or perforation. In some cases, intestinal obstruction is caused by intussusception, but this is an unusual cause of intestinal obstruction in adults, and only few such cases of intussusception caused by RCC have been reported (1-7). To the best our knowledge, multiple small intestinal intussusceptions caused by RCC are extremely rare, and only a case of double intussusceptions involving both the ileum and jejunum has been previously reported (2).
We report here on a case of double jejunal intussusceptions induced by multiple polypoid metastatic lesions from RCC, and this was successfully treated with three segmental resections of the small intestine and functional end-to-end anastomosis.
CASE REPORT
A 47-year-old male patient underwent left radical nephrectomy for a left RCC with metastasis to both lungs (pT1aN0M1) in Sep 2006. There was no lymph node (LN) enlargement or adrenal mass. Histologic examination revealed RCC of the clear cell type, with Fuhrman's nuclear grade III/IV. The size of the tumor was 6.3×5.5 cm, and the renal capsule was involved without penetration. In Dec 2006, a chest CT scan revealed a newly appeared 13-mm sized nodule in the left lung apex. The patient refused further treatment. In Feb 2007, a chest CT scan revealed aggravation of the metastasis in both lungs, and a newly developed left hilar LN enlargement and a right adrenal mass were noted. Palliative sunitinib at 50 mg per day, 4 weeks on and 2 weeks off, was started from Mar 2007. In Apr 2007, a left adrenal mass measuring 2.5 cm in length was newly developed, while the right renal mass increased in size, and there was no interval change in both lungs and the left hilar LN. The sunitinib was stopped and patient refused further therapy. Abdominal pain developed in Jun 2007, and he visited the local emergency room. CT scan revealed enhanced masses with the "target" sign, suggesting enteric intussusceptions in the jejunum (Fig. 1). An emergency operation was recommended, but he refused it and then he visited the Integrative Cancer Center, East-West Neo Medical Center, Kyung-Hee University for a second opinion. The PET/CT scan revealed multifocally increased FDG uptake along the large and small bowel loop areas and viable tumors was thought to be in both adrenal glands, the left paracolic gutter and the left upper lung.
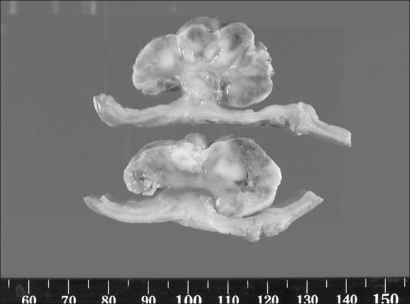
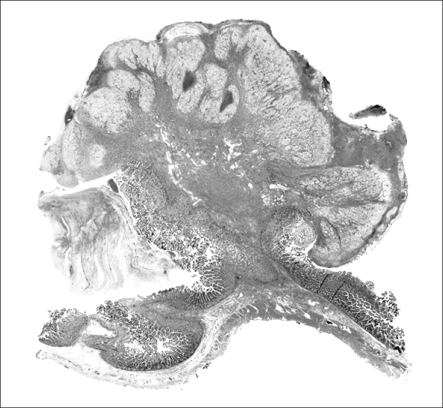
Multiple poylpoid masses in the intussusception segments were found in the resected specimens. These masses led to intussusception at 30 and 150 cm distal to the Treitz ligament. Three segmental resections of the small intestine and functional end to end anastomosis were done at 30, 150 and 250 cm distal to Treitz ligament. The mucosal surface of the small-sized bowel specimen showed a polypoid yellow and greenish mass (4.3×3.5×2.3 cm) The mucosal surface of the medium-sized small bowel showed two polypoid greenish masses (2.5×1.7×1.2 cm and 1.8×1.2×0.5 cm). The mucosal surface of the large-sized small bowel showed five greenish polypoid masses (2.5×1.5×1 cm, 0.7×0.5×0.5 cm, 2.3×1.7×1 cm, 1.4×1×0.5 cm and 2.5×2.2×1.8 cm) (Fig. 2). The cut surface of the polypoid mass was gray white and solid. The polyp had a stalk and surface ulceration (Fig. 3). On the scanning view, a polypoid mass showed ulceration (Fig. 4). Histologic examination revealed that the tumor was composed of clear and granular cells that were surrounded by delicate fibrovascular stroma (Fig. 5). The regional lymph nodes were negative, and a clear resection margin was achieved.
The patient recovered uneventfully from this operation, and he is progression-free for over 10 months after the surgery.
DISCUSSION
The most frequent sites of metastasis from RCC include the lung, lymph nodes, liver, bone, adrenal glands and the opposite kidney (8,9). The incidence of small intestinal metastasis by RCC is reported to be rare. In a report by De Castro, only 3 cases of small intestinal metastasis from RCC for the period of 1905 through 1954 were retrieved from the records of the Mayo Clinic (10). In another report by Smith et al, only one case of small intestinal metastasis from RCC was documented from 1965 to 1975 in the Mayo Clinic (11). In Eggener's study, no small bowel involvement was observed among 118 cases of RCC that recurred after nephrectomy (8). Most of the patients with metastatic RCC in the small intestine also had metastases in other organs (11).
Intussusception is a rare entity in adults and it accounts for one percent of all the cases of bowel obstruction (12). The intussusception in adult patients is often difficult to diagnose preoperatively, and the diagnosis is most often established at the time of surgery. The most useful diagnostic radiological method is computed tomography (CT), which can reveal "target" lesions. According to one study, abdominal CT scans provided a correct diagnosis in 78% of such cases (13).
In a report by Nagorney et al, only 24 cases of adult intussusception originating in the small intestine were documented at the Mayo Clinic between 1955 and 1978. Only one-third of them were harbingers of malignancy, and 70% of these lesions were metastatic lesions (14). Intussusceptions that originate in the small intestine and are caused by RCC have been reported to be rare (2-7,10,14). Among them, only one case presented with multiple small intestinal intussusceptions (2). In our case, eight pedunculated masses within the small intestinal lumen led to intussusceptions at 30 and 150 cm distal to Treitz ligament. To the best of our knowledge, this is the first report of metastases from RCC that presented as synchronous intraluminal multiple polypoid tumors, and these tumors served as the lead points of two intussusceptions in the jejunum.